You're likely juggling two pressures at once right now. One is immediate and personal: keeping nurses, techs, custodial staff, and transport teams safe during fast, messy, high-stress shifts. The other is operational: stopping ordinary trash from being treated like high-risk waste, driving up disposal costs and exposing the facility to preventable compliance problems.
That tension is where medical waste segregation either succeeds or breaks down. The rules can look straightforward on paper, but in a real facility, people make split-second decisions at the point of care. If the system is confusing, inconvenient, or built around fear, staff default to the safest-looking option in the moment, even when it's the wrong one.
A good segregation plan does more than sort waste. It protects workers, supports infection control, preserves treatment capacity, and creates a calmer environment where staff can act with confidence instead of guessing.
Why Medical Waste Segregation Is Your First Line of Defense
A facility manager usually notices the problem before anyone names it. Red bags are filling too fast. Sharps containers are being replaced inconsistently. Housekeeping reports mixed waste in regular trash. Staff say they “didn't want to take chances,” so they threw questionable items into the regulated stream.
That instinct comes from care, but it can create a second problem. Proper medical waste segregation reduces hazardous waste volume by up to 40–60% in healthcare facilities, directly lowering disposal costs because approximately 85% of total healthcare waste is general, non-hazardous waste that should never enter red-bag or incineration streams (WHO health care waste guidance).
The first decision shapes every step after it
Segregation happens at the point of generation. That means the person holding the item decides whether it goes into general trash, a sharps container, a pharmaceutical stream, or a regulated medical waste container. If that first decision is wrong, every downstream process gets harder.
A blood-soaked dressing placed in regular trash creates exposure risk. A clean wrapper dropped into a red bag creates needless treatment cost. A needle forced into the wrong container creates direct injury risk for the next person who touches it.
Practical rule: The safest waste program isn't the one that treats everything as dangerous. It's the one that helps staff identify what is actually dangerous, immediately and correctly.
This is why waste segregation belongs in the same conversation as exposure prevention. Teams working on mastering BBP precautions often improve segregation at the same time, because both depend on clear hazard recognition and consistent point-of-use habits.
Safety, compliance, and cost are tied together
When facilities over-classify waste, they don't just spend more. They blur the line between true biohazards and ordinary refuse. That makes training harder and weakens staff confidence. It also puts pressure on treatment and documentation systems that should be focused on the materials that require special handling.
Facilities that want a stronger foundation should also understand the broader risks and hazards of biohazard waste management, because segregation doesn't stand alone. It affects exposure control, transport, storage, and final disposal.
Understanding the Different Types of Medical Waste
The most common source of confusion is simple: people use the term “medical waste” as if it's one category. It isn't. Some items are ordinary trash. Others require special packaging, labeling, tracking, and treatment because they carry infection, injury, chemical, or environmental risk.
A quick visual can help orient the whole team.
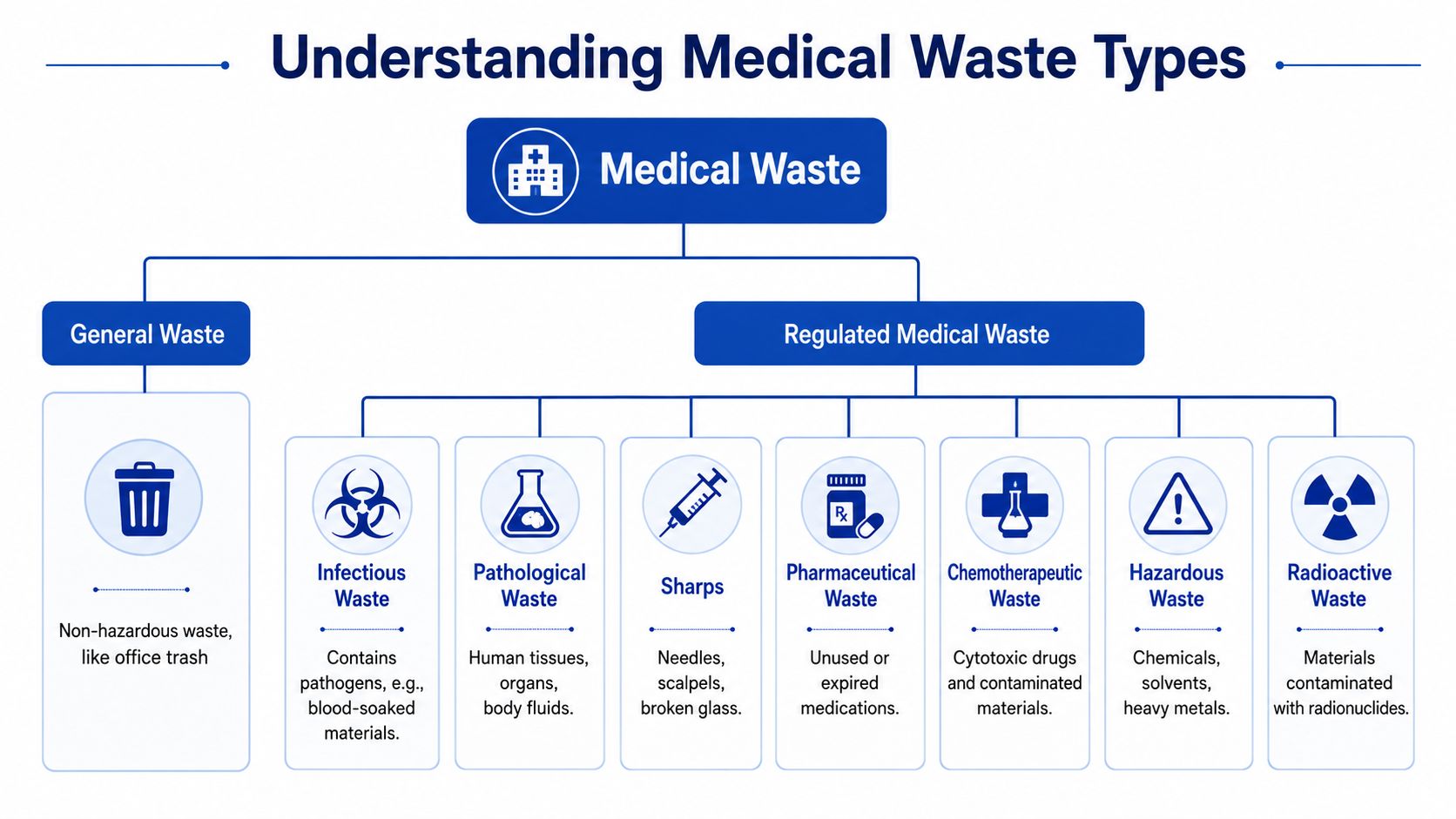
General waste is still most of what a facility throws away
General waste includes non-hazardous items such as office trash and many routine packaging materials. Staff often worry that anything used near a patient must be handled as regulated waste, but that's not how a compliant program works.
If a facility treats ordinary materials as infectious by default, the system becomes expensive and harder to manage. That's one reason practical guidance on how to dispose of medical waste starts with classification, not disposal equipment.
Regulated waste categories exist for different reasons
These categories matter because each one creates a different kind of risk.
- Infectious waste includes materials contaminated with potentially infectious matter, such as blood-soaked items. The concern here is pathogen exposure.
- Pathological waste includes human tissues, organs, and certain body fluids. This category has handling and treatment requirements distinct from general infectious waste.
- Sharps include needles, blades, and other items that can puncture skin. The injury risk is immediate, which is why sharps control is so specific.
- Pharmaceutical waste covers unused, expired, or discarded medications. These materials can trigger regulatory and environmental issues if mixed into the wrong stream.
- Chemotherapeutic waste involves cytotoxic drug waste and contaminated materials associated with those agents. It requires specialized segregation.
- Hazardous waste can include chemicals, solvents, and heavy-metal-containing items generated in healthcare settings.
- Radioactive waste includes materials contaminated with radionuclides and must follow specialized controls.
A simple way to teach the difference
When staff hesitate, teach them to ask one question first: What is the primary risk created by this item?
If the answer is “none beyond ordinary trash,” it doesn't belong in a regulated stream. If the answer is “it can infect, puncture, poison, or contaminate,” then the item needs the correct regulated pathway.
Teams make better decisions when categories are tied to real-world risks, not just memorized labels.
That's why a strong medical waste segregation program doesn't rely on long policy binders alone. It gives people a short mental model they can use at the bedside, in the lab, in environmental services, and in medication areas.
The Color-Coded System A Detailed Breakdown
Once staff understand the categories, they need a system that turns those categories into action. Color coding does that. It reduces hesitation, speeds up decisions, and helps every department handle waste the same way.
Regulated medical waste segregation follows a strict color-coded system: red bags for blood-contaminated items like soaked gauze, yellow bags for pathological waste, blue-marked boxes for glass vials, white translucent puncture-proof containers for needles, and black bags for non-biological medical waste (regulated medical waste disposal methods overview).
Why the container matters as much as the color
A red bag isn't just red. It signals a waste stream that requires controlled handling and treatment. A sharps container isn't just any bin. Its rigid, puncture-resistant construction is part of the safety control.
A common source of trouble for facilities is their focus on poster-based training while forgetting that staff also need the right container in the right place, at the right height, with clear labeling and enough capacity to avoid workarounds.
Medical Waste Segregation Color-Coding Quick Reference
| Container Color/Type | Waste Category | Examples |
|---|---|---|
| Red bag | Blood-contaminated regulated waste | Soaked gauze, visibly contaminated PPE |
| Yellow bag | Pathological waste | Human tissues, certain body-fluid-contaminated dressings |
| Blue-marked box | Glass waste stream | Glass vials, ampules |
| White translucent puncture-proof container | Sharps | Needles, blades |
| Black bag | Non-biological medical waste | Medicine packaging, disposable masks |
Where facilities get confused
People often assume “medical” means “red bag.” It doesn't. A medication wrapper, a dry paper towel from a handwashing area, and office paper are not managed the same way as a saturated dressing or a used needle.
Another point of confusion is container placement. If the correct receptacle is too far away, staff improvise. If labels are vague, people guess. If one unit uses a different convention than another, travelers and float staff revert to the most cautious option.
A facility with high sharps volume should pay close attention to container selection and placement. Detailed guidance on sharps disposal in NYC is a good example of how local handling expectations intersect with universal safety principles.
Clear color coding works best when every bin answers the same question instantly: what belongs here, and what does not?
Navigating Federal State and Transport Regulations
The regulatory environment feels complicated because several agencies govern different parts of the same process. The easiest way to understand it is by role.
OSHA focuses on worker safety. EPA-related requirements focus on environmental handling and disposal issues. DOT governs how regulated waste is packaged, labeled, documented, and transported when it leaves the facility.
DOT rules matter the moment waste leaves your building
This part often surprises managers outside acute care settings. Once regulated waste enters transport, the documentation and packaging standards become more formal.
Regulated medical waste is defined by the Department of Transportation (DOT) as a hazardous material requiring specific labeling, packaging, and documentation, and facilities must use an electronic Manifest system to track disposal from start to finish for transparency and compliance (medical waste regulation processing requirements).
If your team coordinates shipments or vendor pickups, transportation literacy matters. For managers who want a practical overview of DOT hazmat expectations from the fleet side, this ultimate guide for fleet owners gives useful operational context.
Compliance isn't only about bins
A defensible program includes more than visible segregation containers.
- Packaging controls keep waste contained during storage and movement.
- Labeling standards make the hazard obvious to handlers, transporters, and inspectors.
- Manifest tracking creates the chain of custody that shows where the waste went.
- Licensed transport and treatment partners help reduce liability gaps and handling errors.
That's why managers benefit from reviewing broader clinical waste disposal regulations alongside their internal SOPs. The bin is only the beginning. The paperwork, transport handoff, and final treatment pathway matter just as much.
State rules can be stricter
Federal standards set the baseline. States and local jurisdictions may add stricter requirements for storage time, registration, labeling, treatment, or permitted vendors. A plan that looks compliant on a national poster can still fail a local inspection if state-specific details are missing.
The practical answer is simple. Build your facility policy to the strictest applicable rule, then train staff on the version they have to follow on the floor.
How to Implement a Facility Segregation Plan
A workable program doesn't start with posters. It starts with observing how waste is generated in your building. Different rooms, shifts, and service lines create different failure points. A triage room, a behavioral health unit, a dental operatory, a lab bench, and an administrative office do not need the same setup.
Use the infographic below as a planning framework.
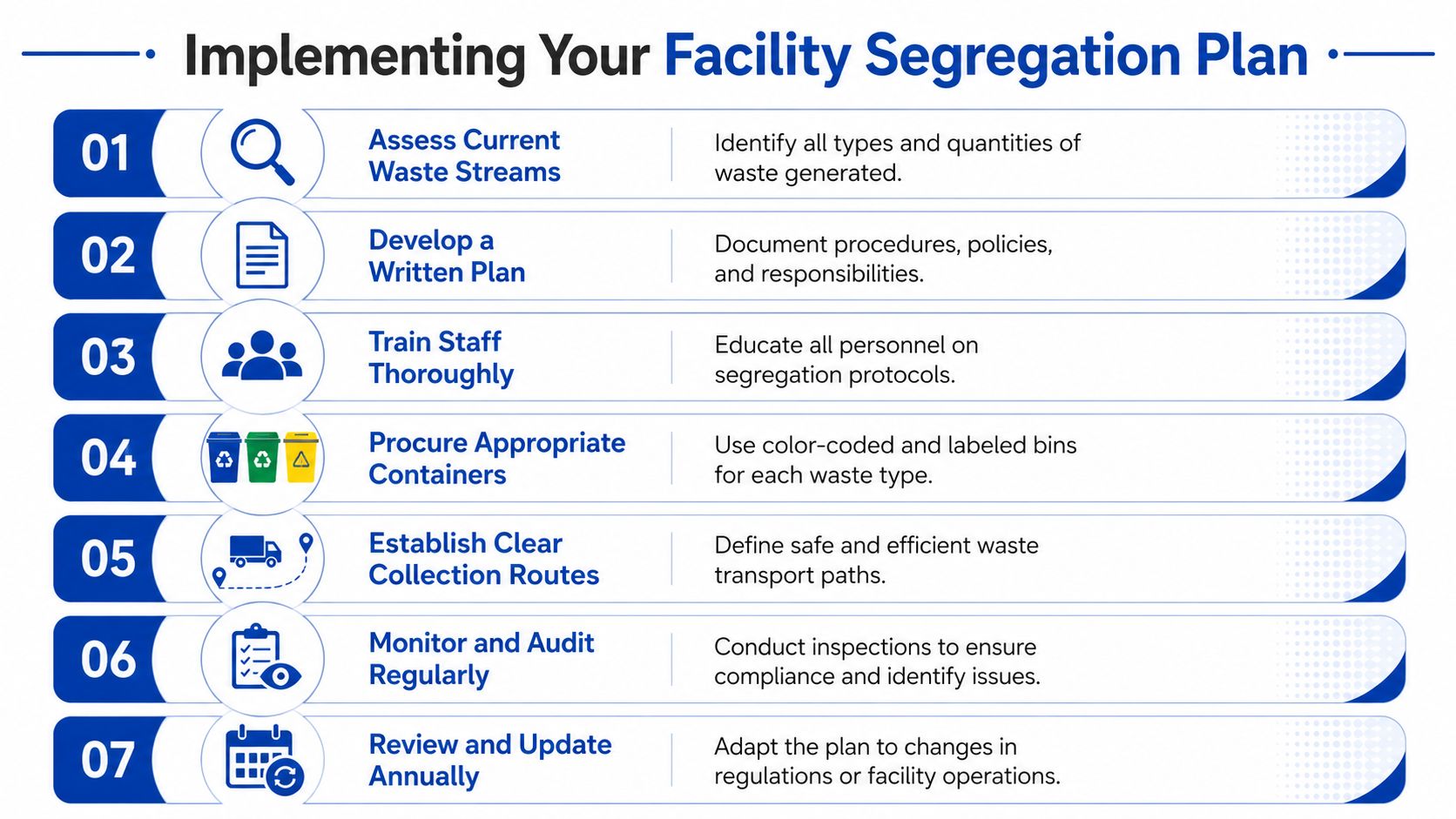
Start with a floor-level waste audit
Walk the facility. Don't rely only on policy documents or purchasing records. Stand where waste is created and watch what staff do under normal conditions.
Look for patterns like these:
- Mismatch between task and container. A treatment room may generate sharps and blood-contaminated soft waste, but only one of those receptacles is available.
- Distance problems. If staff must cross the room or leave a patient area to reach the correct bin, compliance drops.
- Label confusion. Text-heavy labels often fail during busy clinical moments.
- Shift variation. Night staff may follow different habits than day staff because supervision, pacing, and staffing levels differ.
Build the system around the real workflow
A good segregation plan removes friction. It doesn't ask people to remember a complicated chart while they're managing patient care, cleaning bodily fluids, or closing a room quickly for turnover.
That means your written plan should include:
- Waste stream definitions written in plain language.
- Container map by area showing what goes where.
- Visual signage with real item examples, not abstract category names alone.
- Pickup and replacement routines so containers don't overflow.
- Escalation instructions for unusual or uncertain waste items.
This is also where environmental and safety teams should align their practices with broader environmental compliance standards, because segregation decisions affect storage, transport, and final treatment obligations.
Here's a practical training aid that many teams find useful during rollout:
Don't overlook sharps details
Sharps handling is one of the easiest areas to audit because the requirements are concrete. Sharps containers must be puncture-resistant, leak-proof, mounted upright with closable lids, and never filled beyond 75% capacity (indicated by a marked fill line) to prevent needle-stick injuries, which cause 38% of occupational exposures in healthcare waste handling (medical waste disposal stages and sharps guidance).
That single rule has several operational implications:
- Mount containers where the sharp is used, not down the hall.
- Train staff to stop at the fill line, not when the box is visibly crammed.
- Assign replacement responsibility so everyone knows who changes the container and when.
- Inspect mounting stability during rounding. An upright container only helps if it stays upright.
The best segregation plan feels almost obvious to staff because the environment makes the right choice easy.
Audit behavior, not just inventory
Facilities often check whether bins exist. They should also check whether the bins are being used correctly. Open the lid. Review contents. Ask staff why they chose that container. If a mistake appears in three rooms, the problem is probably system design, not individual neglect.
Short, recurring audits work better than one large annual push. They keep standards visible and help managers correct confusion before it turns into routine behavior.
Common Segregation Mistakes and How to Fix Them
The usual explanation for poor segregation is carelessness. That explanation is often wrong, and it leads to weak solutions. Most staff don't mis-sort waste because they don't care. They mis-sort because the moment is rushed, the choice feels risky, and they're trying to avoid making a dangerous mistake.
That's why over-segregation is so common. Research indicates that the root cause for poor segregation is often not a lack of knowledge but a failure to address the 'fear of error' during high-stress events, leading staff to default to 'throw it in the red bag' as a personal risk-mitigation strategy (research on fear of error and segregation behavior).

The mistake behind many other mistakes
When a facility teaches rules without addressing stress behavior, staff often hear this message: If you're unsure, choose the most restrictive option. That may feel safer in the moment, but it trains people to bypass judgment.
A better message is: If you're unsure, use the decision aid posted at the point of care, and escalate unusual items through a clear pathway. That preserves safety without teaching red-bag reflexes.
Practical fixes that work in the real world
Use solutions that reduce cognitive load.
- Replace text-heavy signs with photo-based examples. Show actual items used in your facility, not generic clip art.
- Standardize across departments. A red bag should mean the same thing everywhere in the building.
- Correct overfilling early. Once containers overflow, staff start making workarounds that ripple into other safety failures.
- Train by scenario. Ask staff where they would place a blood-soaked dressing, an empty medication package, a used syringe, or a broken vial.
Compare the mistake to the fix
| Common mistake | Better correction |
|---|---|
| General trash placed in red bags “just in case” | Use point-of-use visuals that define what actually qualifies |
| Wrong container selected during a rushed task | Put the needed receptacle within immediate reach of that task |
| Inconsistent practice between shifts | Audit by shift and retrain with the same examples facility-wide |
| Sharps pushed past fill lines | Assign ownership for replacement before the marked limit is reached |
Staff confidence is a safety control. If people feel forced to guess, the system is underdesigned.
A facility that wants better medical waste segregation should treat human behavior as part of compliance. Fear, time pressure, noise, fatigue, and layout all influence disposal decisions. The strongest programs respect that reality and build around it.
Beyond Compliance Toward a Culture of Safety
Medical waste segregation is one of the clearest signals of how a facility thinks about care. When the system is clear, staff are safer, disposal practices are more defensible, and the organization is less likely to drift into costly, high-risk habits. When the system is confusing, even good people make avoidable mistakes.
A mature program doesn't treat segregation as a housekeeping issue or a poster campaign. It treats it as part of exposure prevention, environmental stewardship, operational discipline, and community responsibility. That's the difference between checking a box and building trust.
Some situations also move beyond routine waste handling. Trauma scenes, severe contamination events, unexpected biohazard releases, and complex remediation needs require trained professionals who understand containment, transport, documentation, and compassionate communication under pressure. That's where specialized support becomes critical, especially when time is short and the consequences are severe.
When your facility needs a trusted partner for biohazard remediation, regulated waste handling support, and compassionate guidance during high-stress situations, 360 Hazardous Cleanup is available to help. Their team brings deep field experience, a compliance-first mindset, and trauma-informed professionalism to complex incidents where safety, discretion, and proper documentation matter most.
