A small clinic finishes a difficult morning. A sharps container is nearly full, a treatment room has blood-contaminated disposables, and a staff member asks the question that stops everyone for a moment: “What exactly are we allowed to throw away, and what has to be tracked?”
A distressed homeowner can end up in the same place after a medical emergency at home. The room is quiet, the materials are unsettling, and the rules feel impossible to sort out under stress.
That confusion is normal. Clinical waste disposal regulations sit at the intersection of infection control, worker safety, environmental protection, and legal liability. They can feel bureaucratic when you first encounter them. In practice, they exist for a very human reason. They reduce the chance that a cleaner, nurse, waste handler, neighbor, or family member gets exposed to something dangerous.
A strong response starts with calm process control. If your team is building or reviewing emergency procedures, this guide to incident management offers a useful framework for documenting who does what, when, and how decisions get escalated. For blood-related events specifically, a written procedure for cleaning blood spills helps turn uncertainty into repeatable action.
Navigating Clinical Waste Disposal After an Incident
The first mistake people make is assuming disposal starts when the waste leaves the building. It doesn't. Disposal starts the moment the material is created.
Take a routine example. A staff member changes a dressing, removes contaminated gauze, and sets aside a used sharp. Nothing dramatic happened. But the next few minutes matter. If those items go into the wrong container, the facility may create a worker exposure risk, a transport problem, and a paperwork problem all at once.
What people worry about first
Most facility managers and property owners ask the same questions:
- What counts as regulated waste: Is it only needles and blood, or also PPE, dressings, and specimen materials?
- Who sets the rules: Is there one national standard, or does your state decide the details?
- What happens if it's handled wrong: Are you dealing with a safety issue, a compliance issue, or both?
The answer is usually “both.” That's why experienced compliance teams don't treat waste handling as housekeeping. They treat it as risk management.
Practical rule: If you can't confidently classify a material, stop and verify before moving it into the regular trash stream.
Why the rules feel so complicated
Clinical waste regulations can seem fragmented because several agencies and state programs influence the process. One set of rules focuses on exposure risk. Another focuses on transport or disposal. Another controls who is authorized to receive the waste.
That can be frustrating when you're standing in a room that needs attention now. But the logic is sound. Each handoff is a point where something can go wrong. The rules build safeguards around those handoffs so risk doesn't spread outward from the original incident.
When readers tell me these regulations feel overwhelming, I usually remind them of one thing. You don't need to memorize every code section to make good decisions. You need a reliable way to sort materials, contain them correctly, document the chain of custody, and use qualified help when the situation goes beyond routine handling.
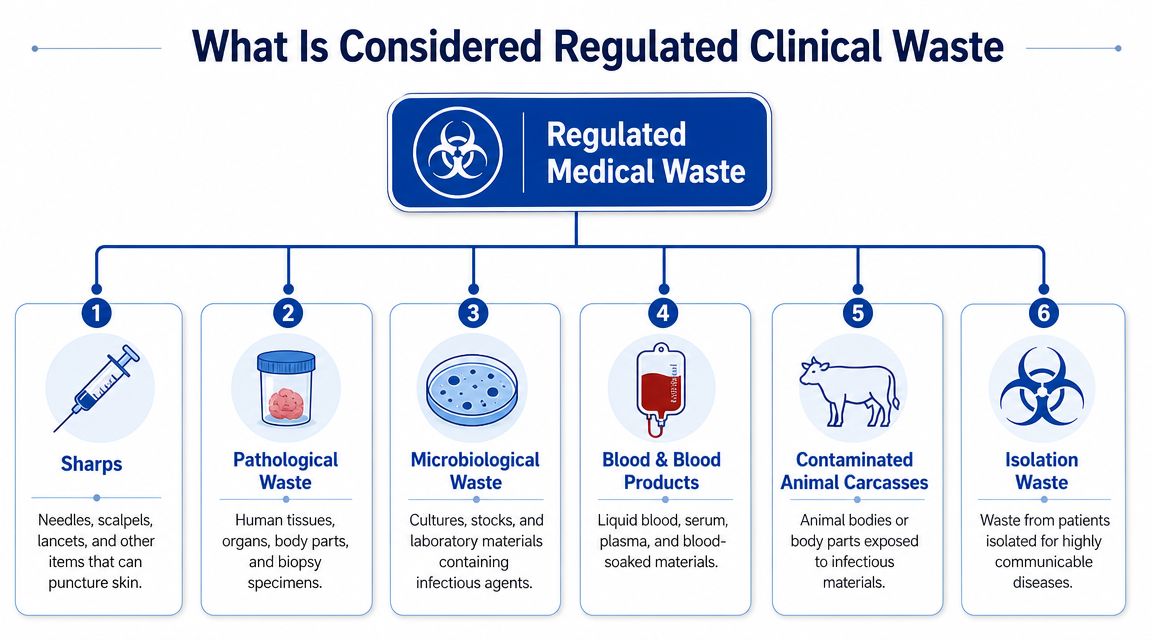
What Is Considered Regulated Clinical Waste
A spill, a used dressing, a blood tube, a full sharps container. In the moment, those items can look like one messy problem. Legally and safely, they are not the same thing. Classification comes first because the disposal path depends on what the material can do to the next person who touches it.
That is the purpose behind the categories. They are not paperwork labels for their own sake. They are risk labels that protect housekeepers, nurses, waste haulers, patients, family members, and anyone else who could be exposed if the wrong item goes into the wrong container.
A useful comparison is kitchen food safety. Raw chicken, a sealed can of soup, and a paper towel may all be on the same counter, but they do not carry the same contamination risk. Clinical waste works the same way. The rule is called source segregation, which means you sort waste where it is created, while the facts are still clear, instead of asking someone downstream to guess.
The main categories people encounter
State programs often use slightly different definitions, but these are the categories facility managers and property owners run into most often:
- Sharps: Needles, lancets, scalpels, and other items that can puncture skin. Their danger is immediate. One wrong grab can become an injury and an exposure event.
- Pathological waste: Human tissues, organs, and materials generated through pathology or anatomy work. These materials require stricter handling because of both infection-control concerns and dignity considerations.
- Microbiological waste: Cultures, stocks, and laboratory items associated with infectious agents. The issue here is not just visible contamination. It is the potential concentration of organisms.
- Blood and blood-contaminated materials: Specimens, containers, saturated dressings, and other items contaminated through handling blood or certain body fluids in regulated settings.
- Contaminated animal waste: Animal carcasses, tissues, or body parts from research or testing when infectious contamination is part of the work.
- Isolation-related waste: Materials generated under added infection-control precautions, where the setting itself signals a higher transmission concern.
One point causes confusion again and again. Not every glove, mask, drape, or empty package from a medical setting is regulated clinical waste. The question is whether the material meets your state's definition for infectious risk, sharps risk, or another regulated category. Over-classifying waste drives up disposal cost. Under-classifying it can expose people to injury, trigger reportable violations, and create liability that is hard to defend after the fact.
That is why careful sorting protects both safety and reputation. If a cleaner is stuck by a needle that should have gone into a sharps container, the problem is no longer limited to disposal. It becomes a worker injury, an exposure investigation, a documentation issue, and potentially a legal one. For readers who want a better grounding in the exposure side of these decisions, this guide to common bloodborne pathogens explains the health risks behind the waste labels.
If you ever need to verify how a term is defined in a statute, rule, or agency manual, the same disciplined method lawyers use can help. This modern lawyer's guide to legal research is a useful reference for checking primary sources instead of relying on informal summaries.
A red bag or sharps container does more than hold waste. It signals hazard to every person in the chain of handling, from the treatment room to final disposal.
Understanding Federal and State Disposal Regulations
One of the biggest sources of confusion is the assumption that the United States has one uniform national rulebook for medical waste disposal. It doesn't.
The EPA explains that the modern U.S. framework was shaped by a major policy shift in 1997, after the federal Medical Waste Tracking Act of 1988 had expired, and that medical waste is now primarily regulated by state environmental and health departments through EPA medical waste guidance. For facility managers, that means the state where the waste is generated usually controls the practical rules for storage, treatment, transport authorization, and disposal.
What the federal agencies do
Federal agencies still matter. They just don't operate as a single all-purpose disposal authority.
A practical way to think about it is this:
| Agency or authority | Main role in practice |
|---|---|
| EPA | Sets the broader environmental framework and explains the federal-state structure |
| OSHA | Focuses on worker exposure, handling practices, and workplace safety expectations |
| CDC | Provides infection-control guidance that shapes how facilities identify and manage risk |
| State health and environmental departments | Define and enforce the on-the-ground disposal program where the waste is generated |
That layered system is why a clinic with locations in different states can't assume one policy manual will cover everything. Container rules, storage limits, recordkeeping expectations, and approved treatment pathways may differ.
Why state-specific compliance is unavoidable
The reason this matters isn't academic. If your team follows a generic national checklist but misses a state-specific requirement, you can still end up out of compliance even if your intentions were sound.
That's why legal and compliance teams often work from primary regulatory text rather than summaries. If you need a useful overview of how to approach statutes, regulations, and official guidance methodically, this modern lawyer's guide to legal research gives a solid framework for tracing authority back to the actual rule.
For workplace-response obligations that sit alongside waste disposal, many facilities also review OSHA guidelines for biohazard exposure and workplace incidents, especially when an event involves employee contact, reporting, or cleanup duties.
Why the history still matters
The EPA also notes that before 1997, more than 90% of potentially infectious medical waste was incinerated. That historical context helps explain why today's regulations care so much about classification, treatment pathways, and downstream handling. The rules weren't written to create paperwork for its own sake. They developed in response to public-health and environmental concerns about uncontrolled disposal and combustion practices.
If your waste policy doesn't identify the state-specific authority that governs your site, it's incomplete even if the rest of the procedure looks polished.
Your Responsibilities as a Waste Generator
A common compliance failure starts with a simple assumption. The waste left your building with a licensed hauler, so the risk must have left with it too.
From a regulator's point of view, your responsibility starts where the waste is created and continues until you can show it was handled, transferred, and documented correctly. That matters for one reason above all others. If something goes wrong later, an injury, a rejected load, a missing container, or an unauthorized transfer, the first question is often whether the generator set up the process safely at the beginning.

Generator responsibility works like signing your name to the first page of a file. Other parties may handle the waste after that, but your decisions at the point of generation shape every step that follows. Correct segregation reduces exposure risk. Correct labeling prevents confusion. Using authorized carriers and receiving facilities lowers the chance that waste ends up somewhere it should not. Good records give you a defensible history if an inspector, insurer, or attorney asks what happened.
What generator responsibility looks like day to day
In practice, this responsibility shows up in routine choices that feel small in the moment but carry real safety consequences:
- Train staff to sort waste correctly at the point of generation: The person finishing a procedure needs to know immediately whether an item belongs in sharps, regulated clinical waste, or general waste.
- Use containers that match the hazard: Needles, blood-soaked materials, specimen-related waste, and breakable contaminated items create different risks and should not be handled as if they are the same.
- Limit access to interim storage areas: Secure storage protects cleaners, maintenance staff, visitors, and contractors who may not expect contact with biohazardous material.
- Confirm that carriers and receiving facilities are properly authorized: A lawful pickup is more than a truck arriving on schedule. The downstream handler must be permitted or otherwise approved under the rules that apply to your site.
- Keep disposal records organized and retrievable: Manifests, pickup logs, weight records, and service documentation help show that the transfer was lawful and complete.
Facilities that want a clearer picture of how exposure risk and compliance connect in daily operations can review this guide to biohazard waste management risks, safety practices, and compliance controls.
Here's a quick visual explainer that many teams find helpful during staff training:
Why documentation protects you
Documentation is what turns a verbal claim of compliance into something you can prove.
Consider a simple example. A container is picked up on Friday, but the receiving facility later reports labeling problems or refuses part of the load. If your team cannot show how the waste was classified, who packaged it, when it was transferred, and which vendor accepted it, the problem can quickly shift from an operational mistake to a liability issue. That can affect inspections, insurance questions, contract disputes, and reputational damage with patients, tenants, or residents.
Good records also protect people, not just organizations. They help trace where a mistake happened so you can correct training, improve storage controls, or change vendors before someone gets hurt.
Key liability point: The safest waste program is one that lets you show who generated the waste, how it was classified, where it was stored, who moved it, and where it went next.
The Process for Safe Containment and Disposal
A disposal process fails long before pickup if the first person handling the waste has to guess.
Safe containment starts at the point of generation because every later safeguard depends on that first decision. The right container protects the person dropping the item in, the custodian who removes it, the driver who transports it, and the treatment facility that receives it. One wrong choice can turn a contained hazard into an exposure event, a reportable mistake, or a dispute over who is responsible.
Step one is matching the waste to the container
Use the container that fits the actual hazard, not the one that happens to be nearby.
Sharps go straight into a puncture-resistant sharps container that closes securely. Soft items contaminated to the level your program treats as regulated waste belong in the designated bag or rigid container for that waste stream. Liquids, specimen materials, and mixed-content items often require special handling based on state rules, local health requirements, and your facility type.
The easiest way to explain this is to compare it to storing household chemicals. You would not pour bleach into a food container and hope the label clears things up later. Clinical waste works the same way. The container itself is part of the safety control.
A used syringe with the needle attached should go directly into the sharps container where it was used. It should not rest on a tray, travel in someone's hand down the hall, or wait for cleanup later. A blood-contaminated dressing that meets your regulated waste criteria belongs in the marked receptacle for that stream, even during a busy shift.
Labels and storage protect the next person in line
Labels are instructions. They tell the next handler what precautions apply before a lid is opened, a cart is moved, or a bag is compacted.
That is why required biohazard markings and state-specific labeling rules matter so much. If a container is not clearly marked, someone downstream may treat it like ordinary trash. The risk then shifts from paperwork to people. Exposure, cross-contamination, and avoidable injury become more likely.
Storage has the same purpose. A proper holding area keeps containers upright, closed, intact, and away from unauthorized access. It also reduces the chance of leaks, tampering, scavenging, or accidental mixing with general waste and supplies.
If your team needs a practical reference for setting up container selection, staging, and service coordination, this guide to biohazard waste disposal procedures can help turn policy into a day-to-day workflow.
Check the hauler before the truck arrives
Your responsibility does not end when a container is sealed. As the waste generator, you still need to know that the transporter and receiving facility are approved for the type of waste leaving your site.
A simple pre-pickup review can prevent expensive problems later:
- Confirm authorization status. Verify that the hauler and destination facility are permitted for the waste stream involved.
- Match paperwork to the actual load. Make sure manifests, pickup logs, or transfer records describe the same category of waste your staff packaged.
- Inspect the handoff area. Staff should know who releases containers, who signs records, and what to do if a package is damaged or the paperwork is incomplete.
This step matters for liability as much as safety. If a vendor mishandles the load, your records and vendor checks help show that your facility followed the required chain of control instead of handing regulated waste to an unknown party.
Many breakdowns here are ordinary and preventable. An overfilled sharps box. A missing label. A storage room left unsecured. A hauler no one properly vetted. Each one creates a weak point in the chain, and clinical waste compliance works like any other chain. The system protects people only when each link holds.
Common Compliance Pitfalls and How to Avoid Them
Most violations don't start with bad intent. They start with rushed decisions, unclear training, or a policy that looks complete on paper but doesn't match what staff carry out.
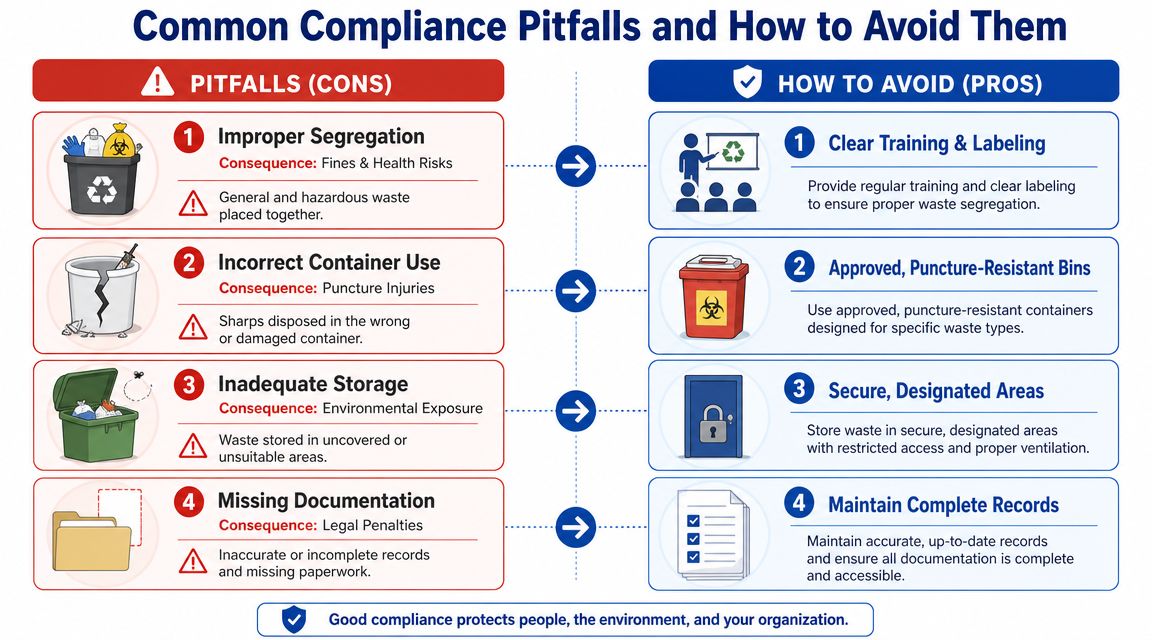
The case of the mixed-up bins
A busy outpatient room uses one red bag for convenience. Staff begin tossing in wrappers, paper towels, and ordinary packaging along with regulated waste.
The immediate harm may not be obvious. But now the facility has inflated a stricter waste stream with materials that didn't belong there. That increases disposal burden and makes audits harder to defend.
Fix: retrain staff at the point of generation, simplify bin placement, and label containers so the right choice is obvious in the moment.
The overfilled sharps container
A procedure area gets hectic. Someone notices the sharps container is near capacity, but replacement is pushed to the next shift. Staff keep using it.
That's how puncture risks rise. The problem isn't just the person dropping in the next sharp. It's everyone who might later move, store, or inspect that container.
Fix: assign replacement responsibility by role, not by assumption. If the fill threshold is reached, the container comes out of service.
The unlocked storage room
A facility designates a waste holding area but treats it like overflow space. Cleaning supplies, spare boxes, and regulated waste all end up there, and the door is sometimes left unsecured.
That setup creates access, contamination, and housekeeping problems at once.
Fix: maintain a dedicated, controlled storage area. Audit it the way you'd audit any safety-critical room.
The missing paperwork file
Pickup happened. The waste is gone. Months later, an internal review asks for manifests, vendor records, and proof of proper transfer. No one can locate the full file.
The disposal itself may have been proper, but now the organization can't prove it.
Fix: centralize records, assign retention responsibility, and review paperwork routinely instead of waiting for an inspection or complaint.
Small process gaps rarely stay small. In clinical waste compliance, a labeling error or missing log can become a worker-safety issue and a liability issue at the same time.
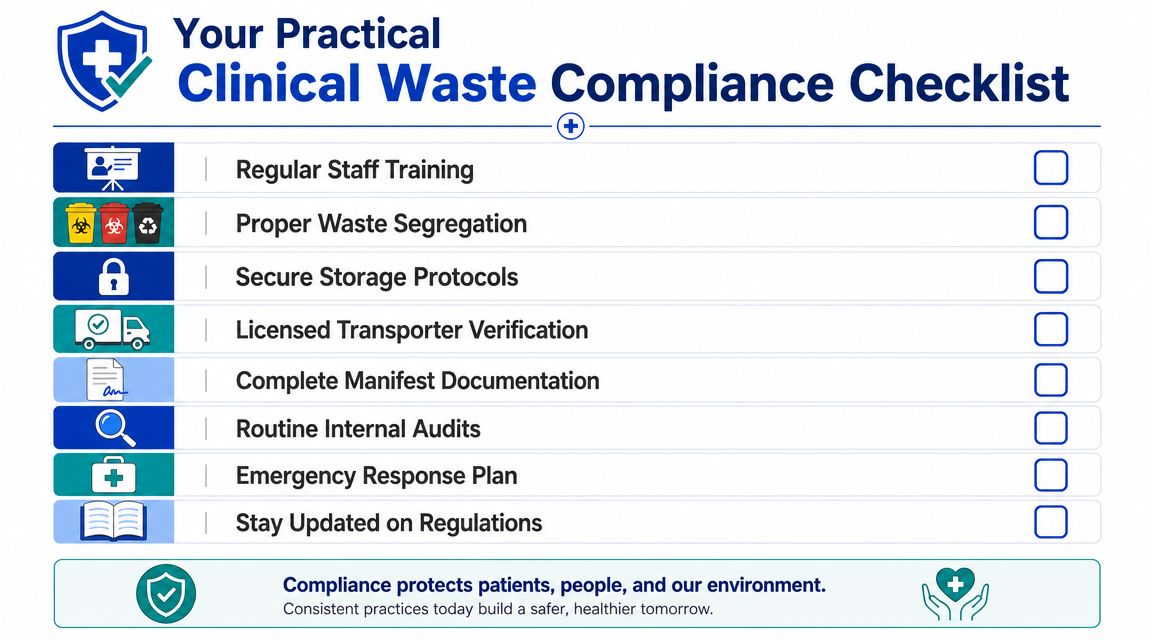
Your Practical Clinical Waste Compliance Checklist
A workable compliance program doesn't have to be flashy. It has to be repeatable. The best programs are the ones staff can follow on a hard day, not just on a calm one.
Use this checklist as a practical self-audit tool:
Daily and weekly checks
- Written procedures exist: Staff know where the waste policy lives and can use it without guessing.
- Segregation happens at the source: Sharps, contaminated soft waste, and general trash are not mixed.
- Containers are appropriate and available: Disposal stations are stocked where work happens.
- Storage areas are secure: Access is controlled and the room is used only for its intended purpose.
Monthly and periodic reviews
- Training records are current: New hires, float staff, and contractors aren't overlooked.
- Vendor credentials are verified: Authorized carriers and receiving facilities are confirmed before service.
- Manifests and transfer records are complete: Paper or digital files are easy to retrieve and review.
- Internal audits are scheduled: Someone checks whether practice matches policy.
Questions that reveal weak spots fast
Ask these in your next walkthrough:
| Question | Why it matters |
|---|---|
| Do staff know what belongs in each disposal stream? | Misclassification starts at the point of generation |
| Can anyone show the last transfer record quickly? | Record control reflects chain-of-custody discipline |
| Is the storage area consistently secured? | Physical access control is part of exposure prevention |
| Are replacement containers available before they're needed? | Delays create shortcut behavior |
If any answer is uncertain, that's useful information. Compliance improves fastest when organizations catch confusion early, before an incident turns into an exposure or an enforcement problem.
Clinical waste disposal regulations can feel dense, but the operational core is straightforward. Identify the waste correctly. Segregate it at the source. Contain it safely. Use authorized transport and disposal pathways. Keep records that prove what happened. That's how facilities protect staff, patients, visitors, the public, and their own reputation.
If you need experienced help building or reviewing a compliant response plan, 360 Hazardous Cleanup provides professional biohazard remediation support with a strong focus on safety, documentation, and regulatory compliance. Their team works with facilities, property managers, and families in high-stress situations where proper handling, lawful disposal, and compassionate communication all matter.
