Healthcare-associated infections affect a significant share of patients worldwide, and the risk climbs in high-acuity units. For hospital leaders, that is not an abstract clinical concern. It is a daily operations issue tied to bed capacity, staff safety, survey readiness, and continuity of care.
Hospital infection control works like a layered defense system. One layer might be hand hygiene. Another is airflow verification. Others include room assignment, cleaning protocols, waste handling, staff training, and documentation that can stand up to regulatory review. If one layer fails, the others have to contain the risk. If several fail at once, a routine room turnover can become an exposure event with reporting, remediation, and staffing consequences.
Facility managers and administrators usually do not struggle with the principle. They struggle with execution. Who confirms negative pressure performance before placement. What level of contamination Environmental Services can clean under existing protocols. Which events require infection prevention, facilities, safety, and clinical leadership to escalate the response together. Those questions sit at the point where policy meets real operations, and they determine whether a facility stays in control or falls behind the event.
That practical gap matters most during high-risk contamination incidents. A blood spill in a controlled area is one thing. A large release involving trauma, sewage backup, isolation failures, or suspected infectious material outside normal cleaning scope is different. Leaders need clear thresholds for internal response versus external remediation support, not just general statements about best practices.
For readers managing risks beyond inpatient units, many environmental controls overlap with other care and commercial settings. A practical reference on organism-specific prevention is this MRSA prevention guidance for facilities, and a broader guide to preventing infections in commercial environments can help teams compare where principles transfer and where hospital standards remain stricter.
The Critical Importance of Hospital Infection Control
Every year, healthcare-associated infections add avoidable illness, longer stays, and heavy operational strain to hospitals around the world. For facility managers and administrators, that reality makes infection control a daily operating requirement, not a background clinical concern.
Hospital infection control covers far more than gloves, sanitizer, and isolation signs. It governs how patients are screened and placed, how airflow and water systems are maintained, how rooms and equipment are cleaned, how waste and linen move through the building, and how leaders respond when contamination exceeds routine procedures. In practice, it works like a chain. A weak link in one department can expose patients, staff, visitors, and the next unit down the hall.
Why the stakes are so high
A preventable infection changes the course of care. A straightforward admission can become a longer, more complex stay with added treatment, delayed discharge, and higher exposure risk for others nearby.
The operational effects spread quickly across the facility.
- Patient safety: Transmission failures can turn recovery into complication management.
- Capacity and throughput: Longer stays reduce bed availability and disrupt scheduling, transfers, and procedural flow.
- Workforce impact: Staff exposures, added PPE demands, and outbreak response duties pull time away from routine care.
- Regulatory and financial risk: Serious lapses can trigger reporting obligations, corrective action, liability concerns, and costly cleanup.
Facility leaders need to read infection control through both a clinical and an operational lens. Academic guidance explains how organisms spread. Daily operations determine whether prevention holds under pressure. That gap matters most during unusual events such as sewage intrusion, a failed isolation room, a large blood or body fluid release, or contamination that extends into HVAC, porous materials, or shared circulation space. In those moments, the central question is not just what the policy says. It is whether the event remains within trained internal response limits or requires escalation to outside specialists.
That is also why mixed-use campuses and medical office environments need clear boundaries between general environmental hygiene and hospital-grade infection prevention. For comparison across settings, this guide to preventing infections in commercial environments can help teams see where practices overlap and where healthcare standards become stricter.
Infection control is a system, not a single team
A strong infection control program depends on coordinated work across registration, nursing, respiratory therapy, EVS, engineering, sterile processing, safety, and administration. Infection Prevention may write the rules and monitor risk, but the facility carries them out hour by hour.
A simple test helps. If a task can move people, devices, air, water, linen, waste, or contaminants, it belongs in infection control planning.
That perspective helps administrators make better decisions about implementation and escalation. Written procedures matter, but so do response thresholds, staffing assumptions, equipment readiness, and communication paths between departments. Leaders should know which incidents EVS can manage under standard protocols, which conditions require infection prevention and facilities review, and which high-risk contamination events call for external remediation support.
Organism-specific planning is part of that work. Teams reviewing contact transmission risks can use this internal resource on MRSA prevention and contamination control to strengthen environmental controls, isolation decisions, and cleaning scope.
Core Principles Standard and Transmission-Based Precautions
Most confusion in hospital infection control comes from mixing up two different layers of practice. One layer applies to everyone. The other activates when a specific transmission risk is known or suspected.
Think of them as universal rules and specialized playbooks.
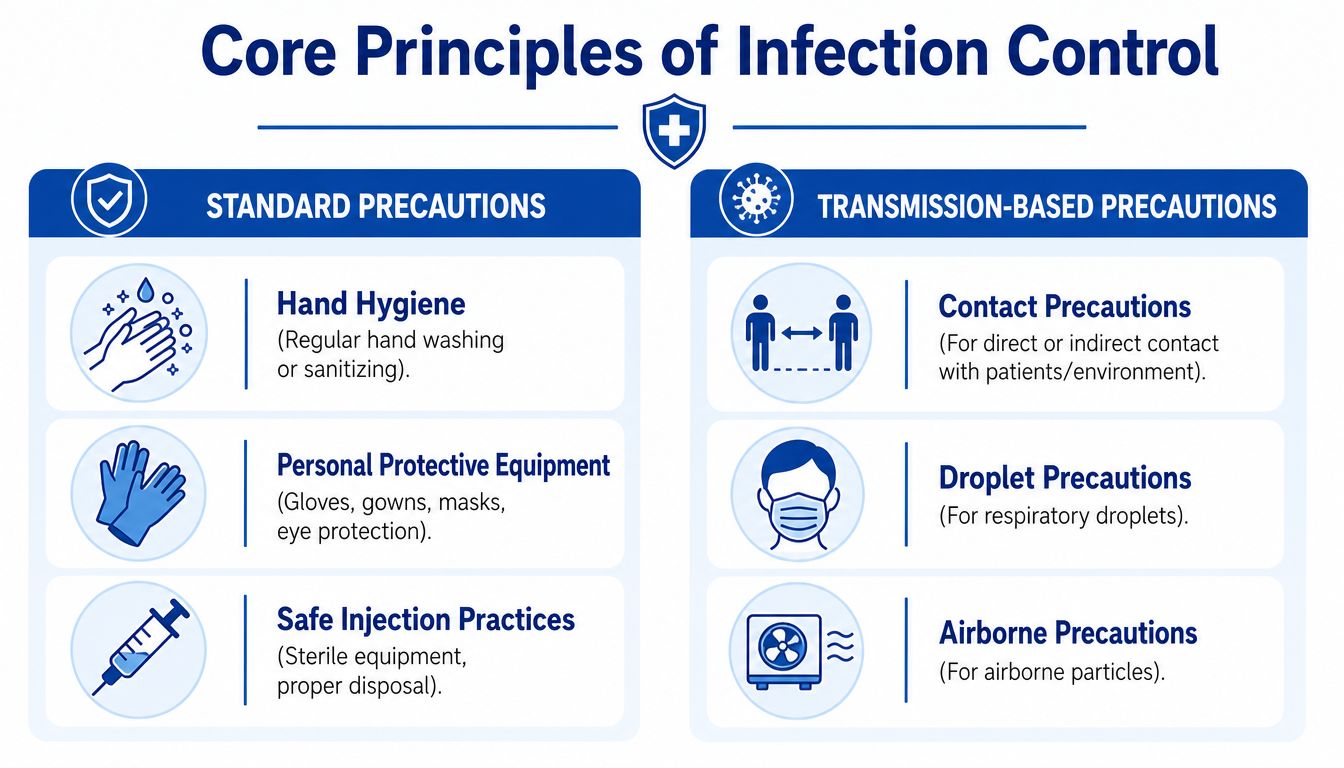
Standard Precautions
Standard Precautions are the baseline used with every patient, every day, regardless of diagnosis. This approach assumes that blood, body fluids, non-intact skin, mucous membranes, equipment, and surfaces may pose exposure risk.
In practical terms, that means staff use risk-based hand hygiene, select personal protective equipment based on the task, handle sharps safely, and follow safe injection practices. For non-clinical leaders, the key point is consistency. A rule that only works when everyone remembers it during a crisis isn't a rule. It's a gamble.
A useful compliance reference for the exposure side of this work is this overview of universal precautions under OSHA, especially for managers responsible for written procedures and staff education.
Transmission-Based Precautions
Transmission-Based Precautions add targeted controls when a patient is known or suspected to carry an infectious agent spread by contact, droplets, or airborne particles.
Here's the simplest way to separate them:
| Precaution type | What it addresses | Operational example |
|---|---|---|
| Contact | Spread through direct touch or contaminated surfaces | Dedicated equipment, gloves, gowns, stricter room-entry workflow |
| Droplet | Spread through larger respiratory droplets | Masking near the patient, rapid placement, transport controls |
| Airborne | Spread through smaller particles that remain suspended | Isolation room controls, respiratory protection, airflow management |
Where non-clinical teams often get tripped up
The biggest misunderstanding is assuming that PPE alone solves the problem. It doesn't. PPE is one part of a larger control package.
A contact-precaution patient, for example, also affects room cleaning chemistry, linen handling, equipment movement, transport pathways, and discharge cleaning expectations. An airborne-risk patient raises an even wider set of questions about room selection, pressure relationships, and engineering verification.
Standard Precautions are the floor. Transmission-Based Precautions are the added controls that match the hazard.
When administrators frame precautions this way, staff make better decisions. EVS understands why a room turn needs different products or more time. Engineering understands why ventilation checks aren't a background task. Unit leaders understand why a placement error can create exposure far beyond one patient room.
Proactive Surveillance and Rapid Outbreak Response
A hospital can't control what it doesn't detect. Surveillance is the facility's early warning system.
In everyday operations, that means collecting signals from lab results, clinical symptoms, patient locations, staff reports, and environmental findings, then turning those signals into action before a cluster becomes a facility-wide problem.
A simple visual helps clarify the cycle.
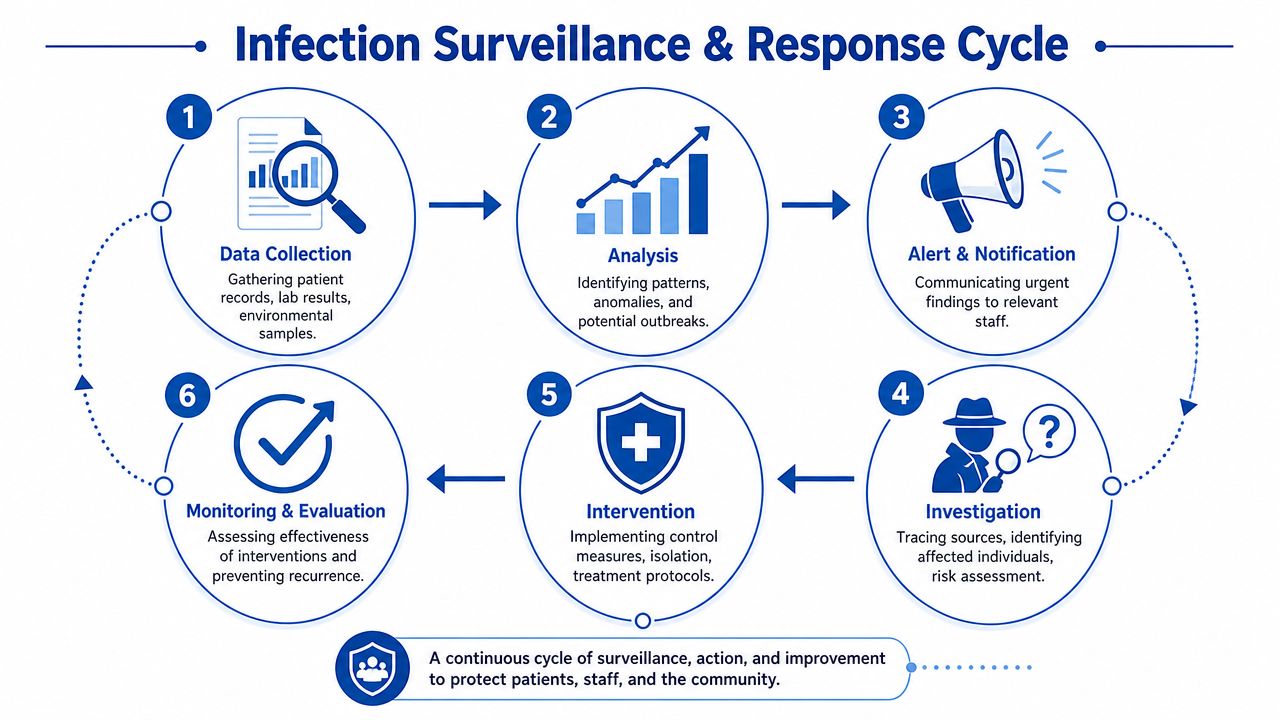
What effective surveillance looks like
Good surveillance isn't passive. Teams don't just collect data and file it away. They ask practical questions.
- Is this infection expected for this patient and unit, or does it suggest transmission?
- Are multiple cases linked by place, time, equipment, or staff workflow?
- Has something changed in cleaning, staffing, patient acuity, or room usage?
That kind of inquiry matters because response speed often determines whether an event stays contained.
According to this review of The Joint Commission's 2024 infection prevention requirements, hospitals must implement six specific protocols for Highly Contagious Infectious Diseases, including screening, isolation, and documented staff competency assessments to support early recognition and minimize transmission.
The first operational moves in an outbreak
Once a cluster looks credible, leaders need a response rhythm. Not panic. Not delay.
The sequence usually includes:
- Confirm the signal: Validate lab and clinical information and define who may be affected.
- Limit spread immediately: Tighten isolation, movement controls, cleaning frequency, and equipment restrictions.
- Notify the right people: Unit leadership, Infection Prevention, EVS, engineering, occupational health, and public health partners when required.
- Investigate the pathway: Look at shared rooms, devices, staffing overlap, transport, workflow shortcuts, and environmental reservoirs.
- Track whether interventions work: If transmission continues, controls need to change.
This short training resource can help teams visualize response discipline in real-world settings:
Why drills matter as much as policies
Many hospitals have an outbreak plan on paper. Fewer have one that people can execute under pressure.
Operations insight: A response plan is only real if staff know who calls whom, where a patient goes, which PPE is needed, what cleaning standard applies, and who documents each step.
That's where competency assessment becomes more than a survey requirement. It becomes a containment tool. The facility that practices screening at entry points, rapid isolation, and clear escalation doesn't eliminate risk, but it reduces confusion at the exact moment confusion causes spread.
The Environment as a Line of Defense
Pathogens don't only move with people. They can persist on surfaces, travel through air pathways, and spread when the built environment isn't performing the way the care model assumes it should.
That's why hospital infection control has to include the physical plant. Clinical skill alone can't overcome a contaminated room, an unverified isolation space, or poor cleaning discipline in high-touch areas.

Cleaning, disinfection, and terminal cleaning are not the same
Facilities often use the word “cleaning” too loosely. From an operations standpoint, these are different activities with different expectations.
| Level | Purpose | Typical use |
|---|---|---|
| Routine environmental cleaning | Remove soil and reduce everyday contamination load | Daily care areas, common touchpoints, support spaces |
| Disinfection | Apply an agent intended to inactivate targeted pathogens on surfaces | Shared equipment, isolation rooms, spill response, high-risk patient zones |
| Terminal cleaning | Perform a comprehensive post-discharge or post-transfer room process | Rooms vacated by patients with known or suspected infectious risk |
If leaders blur these categories, staff start improvising. That usually means missed surfaces, rushed contact times, and inconsistent room turnover quality.
A helpful operational reference for managers coordinating EVS standards is this guide to hospital environmental services and decontamination workflows.
Airflow is an infection control tool
Airborne risk changes everything because the room itself becomes part of containment. For that reason, isolation spaces can't be treated as ordinary patient rooms with a sign on the door.
Per ANSI/ASHRAE/ASHE Standard 170 guidance for health care facilities, Airborne Infection Isolation Rooms must maintain at least 12 air changes per hour and negative pressure, with air exhausted directly outdoors to prevent recirculation.
For facility managers, the practical implications are straightforward:
- Verification matters: A room listed as isolation-capable must perform that way.
- Maintenance matters: Pressure relationships can drift if dampers, filters, or airflow volumes change.
- Documentation matters: When a risk event occurs, leaders need evidence that engineering controls were maintained and checked.
A failed airflow control can turn one isolation room problem into a corridor, adjacent-room, or unit-level exposure concern.
The environment must match the care reality
The safest facilities don't rely on one heroic control. They layer simple, verifiable ones. Clear hand hygiene station placement. Equipment that can be cleaned properly. Isolation rooms that are tested, not assumed. Cleaning workflows that match the patient risk, not the clock on the wall.
When administrators view the environment as a defense system, they fund and manage it differently. That shift pays off in fewer blind spots and better coordination between EVS, engineering, nursing, and Infection Prevention.
Policy Training and Regulatory Compliance
Policies don't protect patients. People using policies correctly protect patients.
That distinction is where many hospital infection control programs either become reliable or remain performative. A binder full of procedures can satisfy a document review. It won't help when a staff member faces a body fluid exposure, needs to don PPE quickly, or has to decide whether a room can safely stay in service.
Compliance starts with usable policy
A useful policy tells staff what to do, who does it, where the equipment is, and what documentation is required. It doesn't bury action steps under vague language.
For hospitals and remediation teams dealing with blood or other potentially infectious materials, a critical regulatory anchor is OSHA's Bloodborne Pathogens Standard. This overview of the OSHA Bloodborne Pathogens Standard requirements explains the need for a written Exposure Control Plan, role-specific risk identification, safety protocols, and post-exposure procedures.
The best policies also account for the fact that different departments encounter risk differently. A nurse, transporter, security officer, maintenance technician, and EVS worker don't need the same script. They need coordinated scripts.
Training has to be active, not ceremonial
Annual education often fails because it becomes a checkbox exercise. Staff sit through slides, sign attendance sheets, and return to the floor without proving that they can perform the task.
A stronger model includes:
- Task-based drills: Donning and doffing PPE, spill isolation, transport controls, waste segregation, and room closure procedures.
- Unit-specific examples: Emergency department screening is different from behavioral health intake or perioperative turnover.
- Competency verification: Supervisors or educators observe the task and confirm that it's done correctly.
- Rapid refreshers: Short updates when guidance changes or when an incident reveals confusion.
Leadership note: If staff hesitate during a high-risk event, the problem usually isn't attitude. It's that the organization trained for recall, not for performance.
Safety culture is part of infection control
Culture sounds abstract until you see what weak culture looks like. Staff stop reporting near misses. Unit leaders normalize workarounds. Housekeeping gets rushed because discharge pressure feels more urgent than decontamination. Engineering concerns are logged but not escalated.
That's why administrators should think beyond technical compliance. They need a reporting culture, reinforcement from managers, and clear permission for any employee to stop a process that feels unsafe. For teams building that foundation, this blueprint for safety culture offers a useful management perspective on how policies become daily behavior.
Regulation should support confidence, not fear
Too many organizations talk about compliance as if the main goal is avoiding a citation. That mindset weakens programs because it narrows attention to inspections rather than operational reliability.
A better view is this: regulations define the minimum structure for safer work. Training gives that structure life. Repetition turns it into habit. Accountability keeps it from slipping when units get busy.
When that human layer is strong, hospitals don't just look compliant. They act prepared.
Auditing Performance and Measuring Improvement
If a hospital doesn't measure infection control performance, it's operating on assumption. Assumption is a poor substitute for evidence.
Auditing turns routine activity into feedback. It shows where policy survives contact with reality and where it breaks down. The goal isn't to generate paperwork. The goal is to catch weak points early enough to correct them.
What to audit in real operations
The most useful audits focus on behaviors and processes that drive transmission risk.
Examples include:
- Hand hygiene observation: Not just whether staff sanitize, but whether they do it at the right moments.
- Room cleaning checks: Whether high-touch surfaces, shared equipment, and discharge rooms meet the expected standard.
- Isolation adherence: Signage, PPE availability, dedicated equipment use, and transport control.
- Engineering verification: Pressure relationships, alarm response, and maintenance documentation for critical spaces.
- Waste handling workflow: Segregation, containment, labeling, transport, and storage practices.
A good audit program also closes the loop. Findings must lead to correction, retraining, redesign, or escalation.
Why reporting systems matter
National reporting systems can feel distant from frontline operations, but they're useful because they create a consistent way to identify patterns and compare performance over time.
The CDC reports that between 2023 and 2024, U.S. acute care hospitals saw an 11% decrease in C. difficile and a 9% decrease in CLABSIs, with progress tracked through systems such as NHSN. That's important because it shows targeted strategies can move outcomes in the right direction when facilities track, review, and act on the data.
Data should answer a practical question: where are we failing, and what change would most likely reduce risk first?
Improvement works best when audits feed CAPA
One of the most common mistakes I see is treating an audit result as the finish line. It isn't. An audit finding is a starting point.
That's where a corrective and preventive action mindset helps. If a team repeatedly misses contact times during disinfection, the answer may not be “train harder.” It may be that the product, staffing pattern, workflow timing, or supervision model is mismatched to the task. This guide to CAPA for regulated environments is a helpful reference for leaders who want a more disciplined response to recurring deficiencies.
A mature audit culture doesn't shame units. It makes problems visible, assigns ownership, and verifies that the fix worked.
When to Engage Specialized Biohazard Remediation Services
Every hospital should have strong internal cleaning and containment capability. Not every event belongs in-house.
That line matters. When leaders ask EVS or unit staff to manage contamination beyond their training, equipment, or regulatory scope, they increase exposure risk for employees, create documentation gaps, and may leave dangerous material behind in places that aren't obvious during a routine cleanup.
The decision point administrators need to recognize
Routine room cleaning, discharge cleaning, and many isolation workflows belong to trained hospital teams. Specialized remediation comes into play when contamination becomes unusually extensive, structurally embedded, operationally disruptive, or legally complex.
The question isn't “Can someone wipe this up?” The better question is “Can our team decontaminate this safely, completely, and in full compliance with the regulations that apply?”
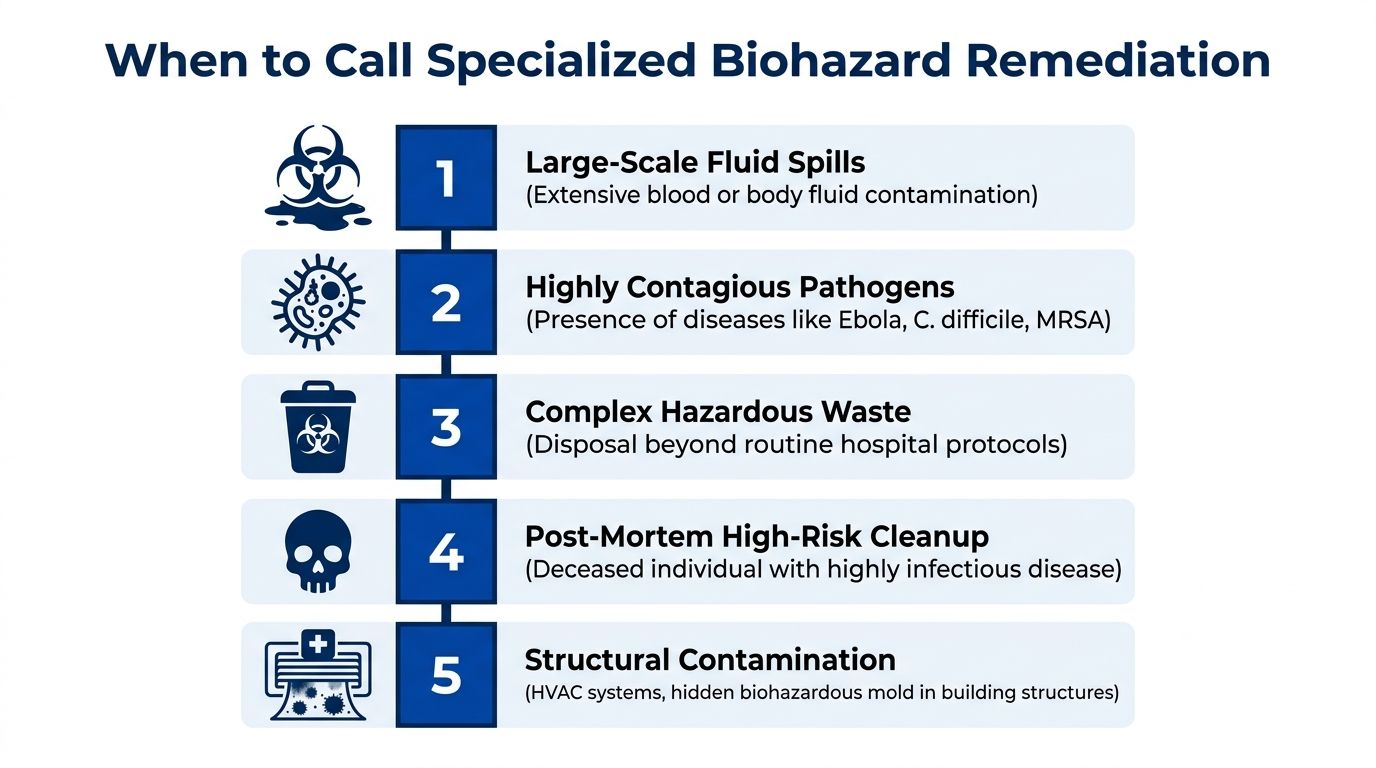
Scenarios that often require escalation
Some situations should trigger immediate consultation with a specialized partner rather than an improvised internal response.
- Large-scale blood or body fluid contamination: Trauma events, severe procedural accidents, or failures involving extensive splash, pooling, tracking, or contamination of porous materials.
- Contamination involving hidden spaces: HVAC components, wall cavities, subflooring, ceiling systems, mechanical chases, or other building areas routine EVS workflows can't fully access or validate.
- Post-mortem or high-risk infectious events: Situations involving remains, prolonged undiscovered contamination, or infectious material that demands a more controlled remediation process.
- Waste and material handling beyond routine streams: Events that generate unusual quantities or categories of regulated waste, contaminated furnishings, or debris requiring specialized packaging and disposal coordination.
- Critical-area restoration: Cleanup after major contamination in surgical support spaces, behavioral health units, isolation infrastructure, or other areas where reopening decisions must be especially defensible.
Escalation rule: If contamination extends beyond visible surfaces, involves worker exposure risk outside routine duties, or affects building systems, stop and evaluate before assigning internal staff.
The OSHA framework is not optional
Biohazard remediation is regulated work. It involves more than "deep cleaning."
According to this summary of OSHA biohazard cleanup requirements under the Bloodborne Pathogens Standard, employers must maintain a written, annually updated Exposure Control Plan that identifies risks, safety protocols, and post-exposure procedures.
That requirement is important for hospitals because it forces leadership to ask several operational questions:
| Question | Why it matters |
|---|---|
| Is this task covered by our written plan? | If not, staff may be operating outside defined controls. |
| Are assigned workers trained for this exposure profile? | Cleanup skill and remediation skill are not always the same. |
| Do we have the right PPE, containment supplies, and disposal pathway? | Missing one element can compromise the whole response. |
| Can we document safe completion? | Reopening a space without defensible documentation creates risk. |
In some aggressive or offensive hazardous response roles, OSHA training expectations can extend beyond basic awareness into specialized levels. Administrators should coordinate with safety and legal teams before assuming an internal crew qualifies for that work.
What specialized partners actually add
A qualified remediation partner brings more than labor. The value is in controlled process.
That includes contamination assessment, work-zone setup, worker protection measures, removal of affected materials when necessary, compliant packaging and disposal, detailed decontamination of impacted areas, and documentation that supports reopening decisions. In healthcare settings, that outside capability can be essential when internal teams need to keep patient care moving rather than diverting staff into unfamiliar high-risk cleanup.
One example is biohazard remediation services for regulated contamination events, which can support facilities facing trauma-related contamination, exposed bodily fluids, infectious material cleanup, or other events that exceed routine EVS scope.
Choosing the right moment to call
The safest time to identify an external remediation partner is before a crisis. Waiting until a severe event occurs usually leads to rushed decisions and uneven communication.
Administrators should predefine call criteria with Infection Prevention, EVS, facilities, risk management, and occupational health. Those criteria might include contamination volume, affected area type, worker exposure concerns, building system involvement, unusual waste complexity, or uncertainty about whether the environment can be returned to safe service by internal staff.
When that threshold is clear, escalation stops feeling like failure. It becomes what it should be: a disciplined risk-control decision that protects patients, staff, and the organization.
Hospital infection control works best when leadership treats it as an operational system with clear limits, clear accountability, and clear escalation pathways. When a contamination event goes beyond internal capability, timely support matters. 360 Hazardous Cleanup provides regulated biohazard remediation and cleanup services for healthcare facilities and other high-risk environments, with an emphasis on safety, compliance, documentation, and compassionate professional response during urgent situations.
