A hospital board often sees Environmental Services when something goes wrong. A room isn't ready. A patient family complains about cleanliness. An inspector asks for documentation. A spill forces a hallway closure. That's understandable, but it misses the bigger truth.
Most of the time, hospital environmental services works best when no one notices it at all. Patients see calm hallways, orderly rooms, stocked dispensers, and surfaces that feel safe to touch. Clinicians see beds turned over on time, isolation rooms handled correctly, and waste removed without disrupting care. Infection prevention teams see something even more important: a disciplined operational function that helps reduce contamination risk every hour of every day.
Boards should treat EVS as part of the hospital's clinical defense system. It sits at the intersection of infection prevention, compliance, labor management, patient experience, and emergency readiness. It also carries financial and sustainability weight. In the 2021 sustainability data from Practice Greenhealth, 269 hospitals reported that their sustainability initiatives in 2020 collectively saved more than $105.2 million, diverted over 204 million pounds of waste from landfill, saved over 31 million gallons of water, reduced more than 78 million kBtus of energy use, avoided more than 78,500 metric tons of carbon emissions, and accounted for more than $566 million in sustainable spending. That scale helps explain why EVS is no longer a back-of-house afterthought.
The harder board-level question isn't whether EVS matters. It's where routine hospital EVS ends, and where specialized biohazard remediation must begin.
The Unseen Guardians of Patient Safety
A visitor walks into a hospital before dawn. The floors reflect the overhead lights. A nurse station is ready for shift change. A patient room has been turned over overnight, the restroom is reset, and the waste stream has been cleared without fanfare. It feels orderly. In healthcare, that feeling matters because order reduces risk.
What is commonly referred to as "clean" in a hospital is the result of controlled, repeatable work performed under pressure. EVS teams don't just make a building presentable. They support patient safety, staff safety, and the reliability of care operations.

Why boards misread the role
The confusion starts with language. "Housekeeping" sounds cosmetic. Hospital environmental services is not cosmetic. It's a specialized healthcare function tied to disinfection, room turnover, waste handling, and infection-control discipline.
That distinction matters because hospitals operate in spaces where a missed high-touch surface, an improperly handled sharps container, or a rushed discharge clean can affect real people. Patients may be immunocompromised. Staff may move rapidly between rooms. Families judge a facility's competence in part by the environment they can see, even though the highest-risk failures are often invisible.
EVS works like a hospital's operational immune system. When it's consistent, the facility feels normal. When it breaks down, the risks spread faster than the mess.
What quiet excellence looks like
Strong EVS performance shows up in ways boards should care about:
- Reliable room readiness: Beds turn over without cutting corners on disinfection steps.
- Calmer clinical flow: Nurses and physicians aren't delayed by avoidable environmental issues.
- Safer shared spaces: Restrooms, waiting rooms, and public touchpoints stay under control.
- Better audit posture: Documentation and protocol adherence are easier to prove.
Facilities that want stronger environmental performance also need staff who understand regulated cleanup standards. Board members looking at competency expectations may find practical context in this guide on biohazard certification for healthcare providers and workers.
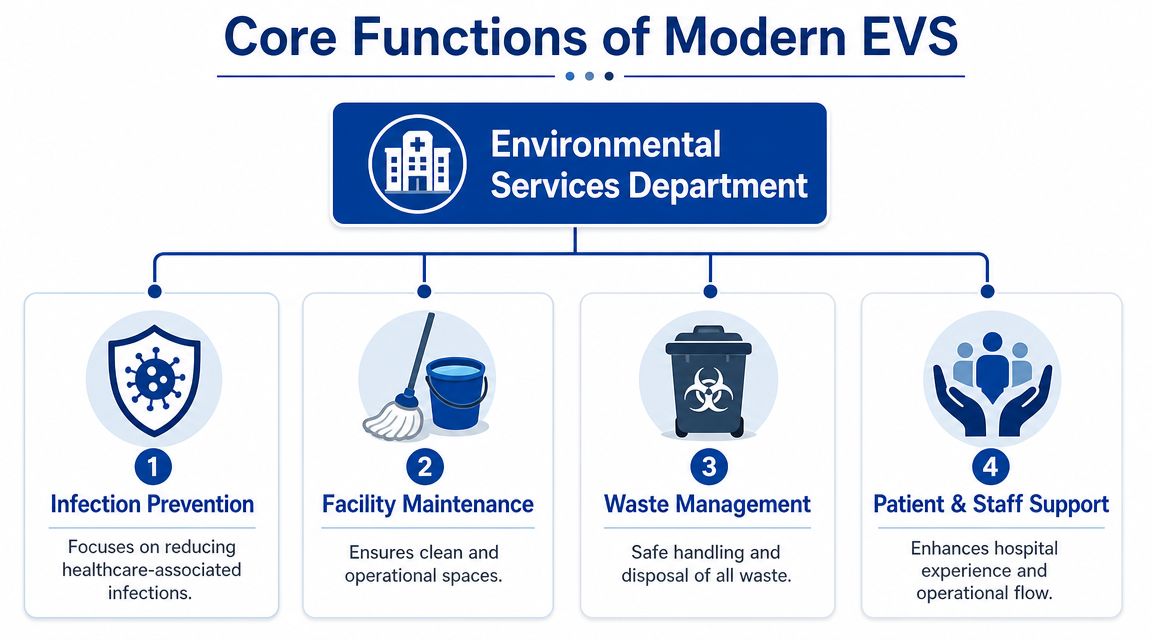
The Core Functions of a Modern EVS Department
Hospital environmental services covers far more than mopping floors and emptying trash. At a minimum, it includes surface cleaning, disinfection, room turnover, waste stream control, support for isolation precautions, and coordination with nursing, infection prevention, and facilities teams.
A useful starting point comes from this overview of what hospital environmental services staff are trained to do. It notes that EVS staff clean and disinfect patient rooms, medical equipment, and shared areas, handle hazardous materials using specialized tools and methods, and that effective room turnover depends on trained staff, proper technique, sufficient contact time for disinfectants, and the right equipment. That last phrase is important. Good outcomes depend on process control, not effort alone.
Cleaning isn't the same as disinfecting
Readers often blur these terms together. In hospitals, that creates dangerous assumptions.
| Term | What it means in practice | Why it matters |
|---|---|---|
| Cleaning | Removes visible soil and organic matter from surfaces | Dirt and residue can interfere with later disinfection |
| Sanitizing | Lowers contamination to a more limited standard | Useful in some settings, but often not enough for patient-care risk |
| Disinfecting | Uses an appropriate product and method to inactivate targeted pathogens on surfaces | This is where infection-prevention value is often created |
A room can look clean and still be poorly disinfected. That's why visual inspection alone isn't a sufficient measure of EVS quality.
The daily responsibilities that shape outcomes
In most hospitals, the modern EVS department supports four practical domains:
- Patient-room care: Daily cleaning, discharge cleaning, restroom service, and attention to high-touch points like bed rails, call buttons, overbed tables, and door hardware.
- Clinical support areas: Emergency departments, procedure spaces, waiting areas, and shared equipment zones need rhythm, prioritization, and coordination with patient flow.
- Waste and sharps handling: Staff must separate general waste from regulated streams and move materials safely through the building.
- Public confidence: Lobbies, corridors, elevators, and visitor areas affect how safe the hospital feels to everyone inside it.
Practical rule: If a task requires the worker to understand contamination pathways, product dwell time, and regulated waste handling, it belongs in a healthcare EVS mindset, not a generic janitorial one.
Boards that want to benchmark whether a team is addressing high-risk pathogens in a disciplined way can use technical resources on cleaning superbugs and infectious bacteria as a useful operational reference.
Standard Protocols for Cleaning and Disinfection
Hospital cleaning fails when people treat it as a checklist instead of a sequence. In patient-care settings, the order of operations matters. Product selection matters. Contact time matters. The worker's technique matters.
The stakes are not theoretical. MarketDataForecast's summary of CDC data says approximately 1 in 31 hospital patients has at least one healthcare-associated infection on any given day. The same source states the U.S. healthcare environmental services market was valued at about USD 6.76 billion in 2024 and is projected to reach USD 9.53 billion by 2029. Growth alone doesn't prove quality, but it does show that hospitals are investing in this function because the operational risk is real.
What proper disinfection actually requires
An effective EVS protocol usually follows a disciplined pattern:
- Assess the space first. Staff identify whether the room is occupied, discharged, under isolation precautions, or affected by visible contamination.
- Remove waste and gross soil. Disinfectants don't work well through organic matter.
- Work from cleaner zones toward dirtier ones. That helps prevent cross-contamination during the task.
- Clean high-touch surfaces methodically. Random wiping misses the surfaces that matter most.
- Honor dwell time. If the product label requires a surface to remain wet for a set period, wiping it dry too early can defeat the claim.
- Use the right tools. Cloth choice, mop system, PPE, and disposal method all affect whether contamination is spread or contained.
Where hospitals get into trouble
The most common misunderstanding is speed. Teams under bed-pressure may feel pushed to turn rooms faster than the protocol allows. A room that reopens quickly but skips contact time or misses shared equipment isn't ready in the infection-control sense.
Another problem is assuming one method fits every event. Routine discharge cleaning is not the same as managing spore-forming organisms, respiratory isolation, or bodily fluid contamination. Facilities facing more severe contamination sometimes need guidance beyond normal EVS playbooks. For broader context on addressing serious property contamination, this external resource offers a useful non-hospital comparison that helps clarify where ordinary cleaning ends and decontamination begins.
Tools support protocol, but they don't replace it
Hospitals increasingly use tools like UV-C support devices, electrostatic application systems, digital checklists, and room-status tracking. Those can help. None of them substitutes for training and execution.
A board-level review should ask simple questions:
- Can the team prove task completion, not just claim it?
- Are high-risk rooms handled differently from low-risk rooms?
- Do supervisors verify technique and chemical use?
- Can the hospital produce a defensible protocol for organisms that require enhanced environmental control?
For facilities struggling with spore-related contamination, a focused operational guide to C. difficile cleaning standards can help clarify why routine disinfection methods aren't always enough.
Navigating Hazardous and Biohazard Waste
Waste management is where many non-clinical leaders discover how technical EVS really is. A trash bag in a patient room may be ordinary solid waste. A red bag in an isolation or treatment area may require a regulated pathway. A sharps container introduces puncture risk, exposure risk, and disposal rules that don't tolerate improvisation.
That is why waste handling belongs in governance conversations, not just loading-dock conversations.
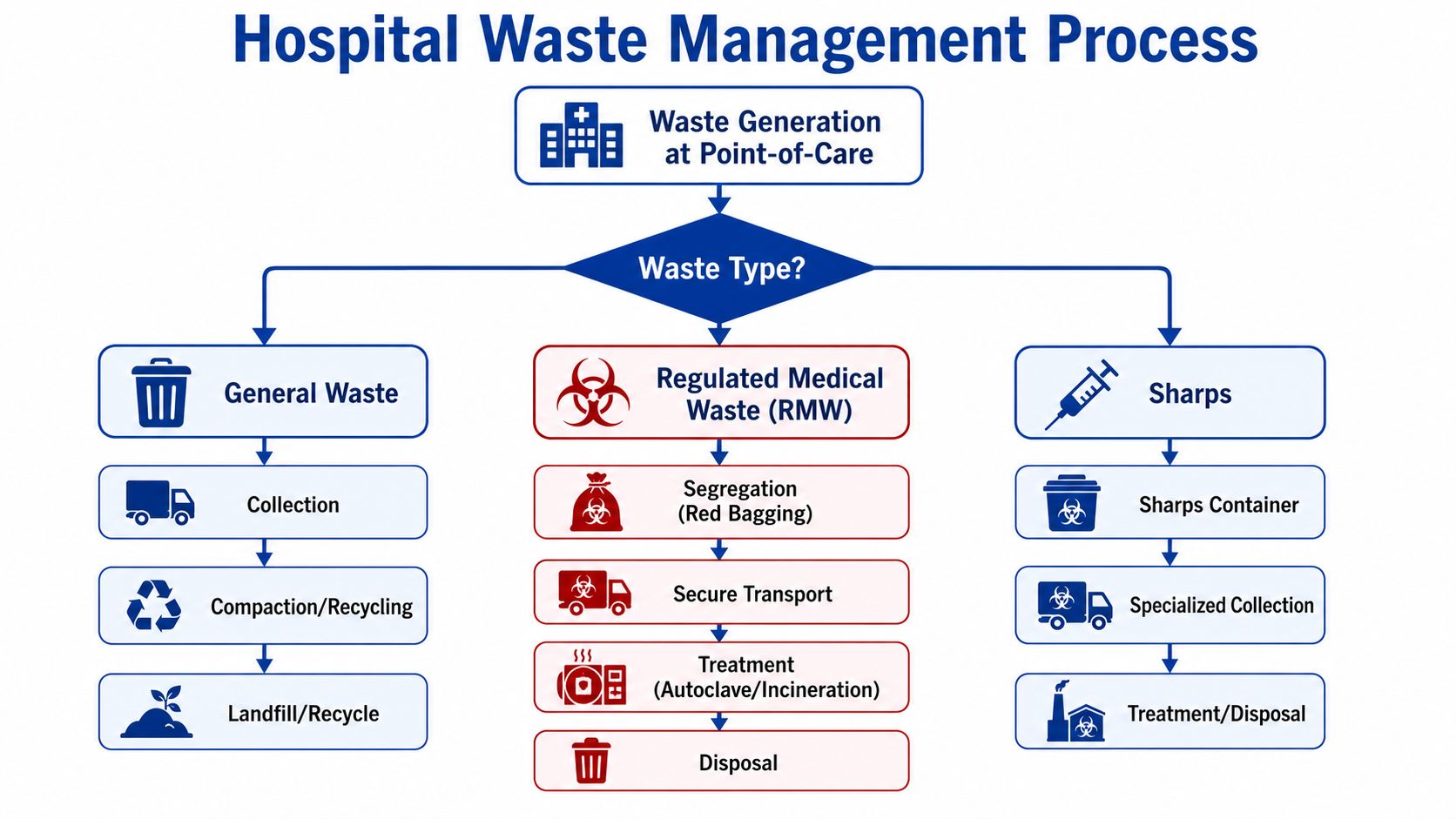
The three streams leaders should separate mentally
Hospital teams often talk about waste as if it's one category. It isn't.
| Waste stream | Typical handling concern | Operational risk if mishandled |
|---|---|---|
| General waste | Standard collection and disposal | Contamination if mixed with regulated material |
| Regulated medical waste | Segregation, containment, secure transport, documented disposal | Exposure risk, compliance failures, reputational harm |
| Sharps | Rigid approved containers and specialized disposal | Needle-stick injuries and bloodborne pathogen exposure |
Each stream needs its own packaging, movement path, and accountability. If staff guess, the system fails.
Why chain of custody matters
The phrase many administrators need to remember is simple: once hazardous material enters a regulated stream, the facility's responsibility doesn't end at the room door. It continues through internal handling, storage, transport, treatment, and final disposal according to applicable requirements.
This overview is worth watching because it helps non-EVS leaders visualize how medical waste segregation affects the whole operation.
Hospitals reviewing staffing exposure and outsourced support arrangements may also benefit from this external Guide to biohazard cleanup PEO risk, especially when evaluating how worker risk, insurance, and vendor oversight intersect.
A waste mistake is rarely just a housekeeping mistake. It can become a worker injury, a reportable event, a contractor dispute, or a regulator's question.
When in-house EVS is enough and when it isn't
Most daily waste segregation tasks belong with trained in-house EVS staff. They should manage point-of-use collection, movement through approved internal routes, and coordination with licensed downstream disposal partners.
Specialized backup is the safer choice when the event includes bulk blood, trauma-related materials, unknown biological contamination, unattended death conditions, or mixed hazards that exceed ordinary hospital waste protocols. In those cases, a provider with documented procedures for biohazard waste disposal can help reduce legal and exposure risk.
The Regulatory and Accreditation Maze
Compliance pressure on EVS doesn't come from one source. It comes from overlapping expectations. Worker safety rules affect PPE and exposure response. Disinfectant rules affect what products can be used and how. Accreditation standards affect documentation, consistency, and readiness for survey.
That overlap is why weak EVS programs often fail internally before they fail publicly. The floor may look acceptable while the documentation, product use, or room-tracking record falls apart under scrutiny.
What regulation looks like on the ground
For leaders, it helps to translate agencies into daily tasks:
- OSHA concerns usually show up as worker exposure controls, PPE practices, bloodborne pathogen precautions, and spill response expectations.
- EPA-related concerns often appear in disinfectant selection, label compliance, and certain waste-handling obligations.
- Accreditation pressure shows up in evidence. Can the hospital show what was cleaned, how, by whom, with what product, and under what protocol?
A modern EVS operation increasingly uses technology to make those answers easier to verify. According to the MarketsandMarkets overview of the U.S. healthcare environmental services market, the sector is being modernized with automated and IoT-enabled cleaning technologies and real-time management tools, and acute-care facilities represented the largest sub-segment in 2023. That matters because acute-care environments tend to carry the tightest turnover and protocol pressures.
Why digital oversight is becoming standard
A clipboard can document a task. It can't easily validate execution across a complex hospital. Digital systems can improve visibility by tracking room status, assigning workflows, time-stamping completion, and helping managers spot missed steps or recurring bottlenecks.
That doesn't mean software creates compliance. It means software makes compliance easier to supervise. The board's interest should be simple: can leadership prove disciplined execution during a survey, complaint, outbreak review, or exposure investigation?
Survey readiness isn't a once-a-year cleaning sprint. It's the daily ability to show that protocols were followed when no one thought they were being watched.
Hospitals that need a plain-language compliance baseline for high-risk cleanup should review biohazard remediation laws and regulations, especially when comparing ordinary EVS duties with remediation-level events.
Best Practices for EVS Staffing and Training
An EVS program rises or falls with its workforce. Policies don't clean rooms. Training documents don't manage a blood spill. People do. If the hospital treats EVS labor as interchangeable, the program becomes fragile.
Peer-reviewed commentary in this article on EVS worker protection and patient care value argues that EVS should be treated as a core patient-care investment, not a peripheral expense. It also states that EVS workers need sufficient PPE and continued innovation to improve their effectiveness. That's an operational point, not a symbolic one.
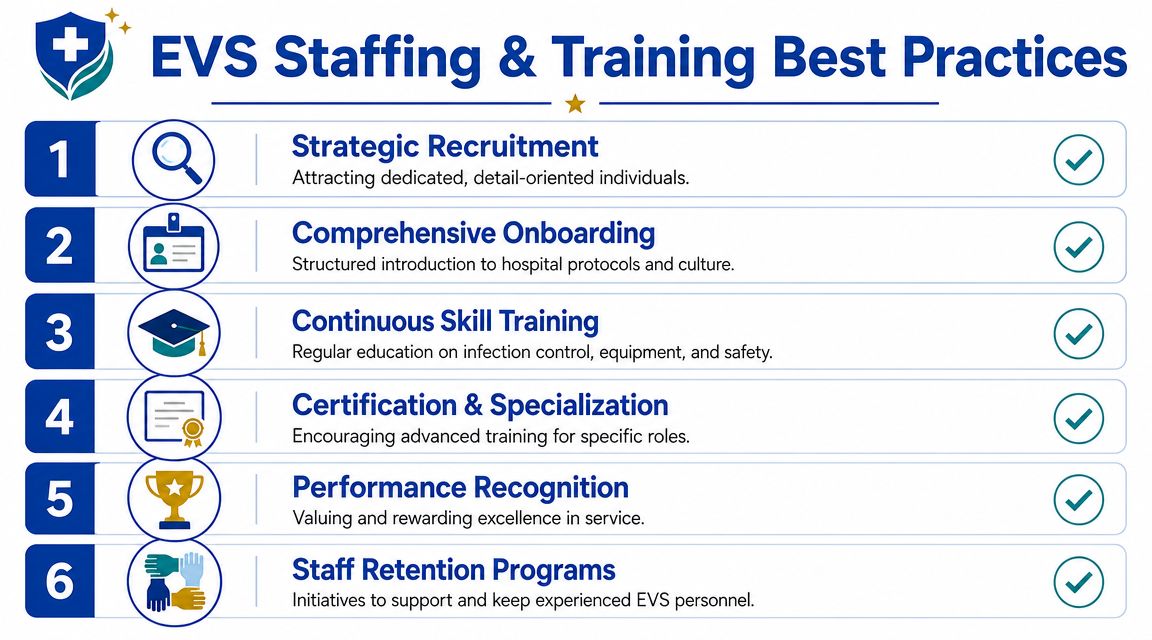
What a durable staffing model includes
Hospitals don't need perfection. They need stability, competency, and supervision.
Consider these staffing priorities:
- Role-specific onboarding: New hires should learn room types, cleaning sequences, waste streams, PPE expectations, and escalation triggers before they work independently.
- Hands-on validation: Managers should watch technique, not just confirm attendance at training.
- Pathogen-aware education: Teams need different procedures for routine discharge cleaning, isolation support, and visible bodily fluid events.
- Human-skills training: EVS staff work around vulnerable patients, stressed families, and confidential care activity. Discretion matters.
- Supervisor development: A strong frontline lead can catch drift before it becomes a safety event.
Worker protection isn't optional
Some boards underestimate how physically and emotionally demanding EVS work can be. Staff move quickly, handle unpleasant materials, encounter grief, and absorb pressure from every direction when census is high. If leadership under-equips them or leaves them out of planning, quality slips first and retention problems follow.
A practical way to think about training is to separate three levels of readiness:
| Readiness level | What staff should handle | What requires escalation |
|---|---|---|
| Routine EVS | Daily cleaning, discharge cleaning, basic waste handling, standard room turnover | Any event outside established protocols |
| Enhanced EVS | Isolation support, higher-risk disinfection workflows, close coordination with infection prevention | Severe contamination, trauma, unknown hazards |
| Specialized remediation | Not an in-house default role | Scenes involving significant biohazard load, trauma, or mixed-risk exposure |
Hospitals do best when they support EVS workers as professionals, not just labor. That means PPE availability, realistic workloads, refresher training, incident debriefs, and a clear path to call for help without stigma.
Emergency Coordination and Specialized Biocleanup
At 2:10 a.m., a patient transport route is suddenly closed after a traumatic blood release extends from an elevator into a hallway and touches more than one surface type. Nursing needs the path reopened. Security needs access controlled. EVS needs direction. In moments like this, the board is not judging whether the hospital can clean. It is judging whether the hospital can recognize when cleaning has become incident management.
That distinction protects people and the institution.
As noted earlier, outside commentary on hospital EVS during respiratory-risk events shows how far in-house teams already stretch during isolation support, outbreak response, supply coordination, and infection-prevention workflows. Those expanded duties still do not make every contamination event an EVS assignment. A hospital room turnover follows a playbook. A trauma scene, an unattended death condition, or an exposure with unclear spread behaves more like a chain-of-custody and risk-control problem.
Incidents that usually exceed routine EVS scope
Hospitals should consider specialized biohazard support when an event includes any of the following:
- Trauma-related bloodshed: Emergency department incidents, violent events, or scenes with significant bodily fluid contamination.
- Unattended death conditions: Especially in hospital-owned housing, off-campus facilities, or non-clinical areas where decomposition or advanced contamination is present.
- Large contamination footprints: Hallways, elevators, transport routes, or exposure across multiple rooms.
- Unknown biological risk: Cases where the source, age, or spread pattern of contamination is unclear.
- Mixed hazards: Biological contamination combined with chemicals, damaged porous materials, or areas connected to HVAC flow.
The practical question is not whether the in-house EVS team is dedicated or skilled. It is whether the event has crossed into a category that requires different PPE decisions, waste handling, containment methods, documentation, and emotional safeguards for staff.
A simple decision test for leaders
Use three questions:
- Can our EVS team identify the hazard with confidence?
- Do they have the PPE, training, and waste pathway to remediate it safely?
- Can we document the response to a standard we would defend to a regulator, in litigation, and in front of a grieving family?
A single "no" should trigger escalation.
Boards sometimes hesitate here because calling a specialist can feel like admitting a gap. The better frame is surge capacity with a narrower scope. In-house EVS handles the hospital's daily environmental control. A specialized remediation firm steps in when the event carries higher exposure risk, unusual contamination patterns, forensic sensitivity, or disposal complexity that falls outside normal hospital cleaning operations.
One option hospitals use for these escalation scenarios is 360 Hazardous Cleanup, a biohazard remediation service that handles trauma, bodily-fluid, infectious disease, and other hazardous contamination events. The selection standard is straightforward. The outside team must work safely, discreetly, and inside the hospital's incident command, security, infection-prevention, and documentation requirements.
Selecting a Qualified Biohazard Remediation Vendor
Vendor selection goes wrong when facilities wait until after the event. By then, the pressure is emotional, operational, and reputational. A better approach is to prequalify one or more remediation partners before the hospital needs them.
The right questions are practical.
What to verify before signing anything
- Training and regulatory alignment: Ask how the company trains for bloodborne pathogen exposure, PPE use, hazardous waste handling, and scene-specific decontamination.
- Insurance detail: Confirm that coverage fits pollution and contamination risk, not just general liability.
- Written scope of work: The vendor should explain what it will remove, clean, disinfect, document, and dispose of.
- Waste handling process: You want a clear answer on packaging, transport coordination, and disposal documentation.
- Discretion standards: Hospitals need vendors that understand privacy, controlled access, and patient-family sensitivity.
- Operational coordination: The company should be able to work within hospital command structures, security procedures, and off-hours access requirements.
Questions worth asking in plain language
Instead of asking whether a company is "qualified," ask things like:
| Ask this | Why it matters |
|---|---|
| What incidents do you consider outside normal janitorial or EVS scope? | It reveals whether they understand escalation thresholds |
| How do you protect workers and nearby occupants during active cleanup? | This exposes their safety discipline |
| What documentation do you leave behind? | Records matter after the scene is gone |
| How do you handle compassion and privacy during trauma-related events? | Technical skill without sensitivity can create new harm |
A good vendor lowers uncertainty. A poor one transfers it.
Hospitals should also decide in advance when in-house teams remain sufficient. Routine room turnover, standard discharge cleaning, and ordinary regulated waste segregation generally belong with trained EVS staff. Events involving trauma, significant blood or bodily fluids, decomposition, unknown contamination pathways, or mixed hazards should trigger specialist review. That line protects workers, patients, and the institution itself.
If your facility needs a response partner for incidents that fall outside routine hospital environmental services, 360 Hazardous Cleanup offers 24/7 biohazard remediation, infectious disease disinfection, trauma cleanup, and regulated waste handling support. For hospitals, clinics, behavioral health sites, and other healthcare properties, the value is straightforward: a trained outside team can step in when the contamination risk, documentation burden, or human sensitivity of the event exceeds what an internal EVS team should reasonably be asked to manage.
