A room can look clean and still leave everyone uneasy.
That happens after trauma scenes, infectious disease exposure, sewage backups, and even some medical incidents. The visible material is gone. The odor may be reduced. Surfaces may even shine. But the essential question stays the same for the property manager walking the site or the family standing in the doorway. Is it completely safe now?
That gap between looking clean and being safe is where UV light disinfection often enters the conversation. People hear about UV devices in hospitals, see handheld wands online, or assume a bright lamp can finish what mops and chemicals started. Sometimes it can help. Sometimes it cannot. The difference comes down to science, measurement, and disciplined remediation practice.
In professional biohazard work, UV isn't a shortcut. It's a terminal disinfection tool used in carefully selected situations after physical contamination has already been removed and after manual cleaning has addressed what light can't. That distinction matters because pathogens don't care about marketing language. They respond only to dose, surface conditions, line of sight, and operator competence.
A similar principle applies after other property damage. For example, when moisture gets into walls, replacing materials correctly matters as much as surface appearance. A practical guide on how to repair water damaged drywall is useful because it shows that restoration isn't cosmetic. It depends on what remains inside the structure, not just what you see from the doorway.
The same is true here. UV can be powerful, but it can also be oversold, misapplied, or used in ways that create a false sense of safety. In high-stakes environments, that false confidence is dangerous. People re-enter rooms. Staff return to work. Families sleep there. Patients receive care there.
Introduction The Unseen Threats After Cleanup
A facility manager usually notices the problem first in the quiet moments after the crew leaves. The caution tape is down. The waste is removed. The room is back in serviceable shape. But there are still touchpoints, seams, fabrics, air movement patterns, and surfaces that were near contamination.
Families feel it differently. They don't use the phrase "terminal disinfection." They ask whether the bedroom is safe, whether the bathroom can be used, or whether a child can go back into the room. Those are fair questions, and they deserve precise answers.
Why a clean room can still feel uncertain
Biohazard cleanup isn't only about appearance. It involves removing contamination, reducing pathogen load, following disposal rules, and restoring the environment to a condition people can safely re-enter. UV belongs near the end of that process, not the beginning.
Practical rule: If a space still has visible soil, residues, dust, or bodily fluid contamination, UV isn't the next step. Manual cleaning is.
That point gets lost because UV is easy to describe and hard to apply well. A lamp feels simple. Actual disinfection isn't. Professionals treat UV as one layer in a broader risk-control plan, especially in medical, commercial, and trauma-related settings where mistakes affect many people.
Where UV fits in the real world
In the best cases, UV adds value after the hard work is done. It can support final surface disinfection in rooms that have already been cleaned and prepared. In the wrong hands, it becomes a gadget that shines on surfaces without delivering a verified germicidal result.
That difference is one reason experienced remediation teams don't treat every job the same way. A patient room, a warehouse restroom, an apartment after an unattended death, and an ambulance bay each present different materials, obstructions, and exposure concerns.
How UV Light Inactivates Dangerous Pathogens
"UV light" is a broad term. For disinfection, the important band is UV-C.
According to Stanley Electric's explanation of UV-C disinfection, ultraviolet germicidal irradiation uses UV-C wavelengths between 180 and 280 nm to inactivate microorganisms by damaging DNA and RNA, with peak disinfection efficiency at 265 nm. That same source notes that 265 nm is over 1,000 times more effective than UV-A and over 50 times more effective than UV-B. That is why not every ultraviolet product is a germicidal product.

What UV-C is actually doing
Think of a pathogen as carrying a set of instructions. Bacteria and viruses rely on genetic material to reproduce. UV-C light damages that instruction set, so the organism can't keep replicating normally.
That doesn't mean the light "washes" a surface. It doesn't dissolve grime. It doesn't lift residues. It doesn't remove blood, tissue, or organic debris. It works by delivering energy that disrupts the microbe's genetic material.
For facilities dealing with persistent infection concerns, topics like MRSA prevention in shared environments often intersect with this issue because high-touch surfaces can carry risk even after routine housekeeping if the overall infection-control plan is weak.
UV-A, UV-B, UV-C, and far-UV-C
Readers often lump all ultraviolet light together. That creates confusion fast.
| Type | General role in this context | Key takeaway |
|---|---|---|
| UV-A | Not the primary germicidal band | Too weak for serious surface disinfection claims compared with UV-C |
| UV-B | More energetic than UV-A | Still far less effective than UV-C for germicidal work |
| UV-C | Main germicidal range | The band used for microbial inactivation |
| Far-UV-C | Emerging area, often discussed around 222 nm | Promising in some controlled applications, but still requires careful safety review |
Why bright light isn't enough
A bright lamp can look impressive and still fail microbiologically. Germicidal success depends on using the right wavelength and delivering the right dose to the right surface.
UV disinfection is a biophysical process, not a visual one. The room doesn't become safer because it looks illuminated.
That is why professionals ask technical questions first. What wavelength is the device producing? What is the measured intensity at the target surface? How long is the dwell time? What areas are shadowed? Those questions matter more than the product box.
Dose and Efficacy The Critical Variables
The central equation is simple. Dose = intensity × time. The field application is not simple at all.
As explained by StellarNet's overview of UV disinfecting lamps, UV-C germicidal irradiation must deliver a specific ultraviolet dose calculated as intensity in μW/cm² multiplied by exposure time in seconds. The same source states that inactivating viruses on ideal flat surfaces generally demands a minimum threshold of at least 40 mJ/cm² to ensure complete genomic damage preventing replication.
Why dose matters more than device ownership
Owning a UV unit doesn't tell you whether a surface received a useful germicidal dose. Two identical rooms can produce different results because of lamp placement, wall reflectivity, clutter, and distance from the source.
That matters in healthcare and high-risk commercial settings, where infection control procedures in occupied facilities require repeatable, validated methods rather than assumptions.
A common failure point is distance. The farther the target is from the lamp, the lower the delivered intensity becomes. In practical terms, a surface close to the unit may receive a meaningful dose while a surface across the room may receive very little, even during the same cycle.
A plain-language way to think about intensity and time
Use a flashlight analogy, but with higher stakes. A beam close to the wall looks strong. Move the wall much farther away and the light spreads out. The energy at any one spot drops.
For UV disinfection, that means:
- Close surfaces may get enough dose during the set cycle.
- Distant surfaces may need far longer exposure.
- Obstructed surfaces may receive almost none.
The same source from Stanley Electric gives a practical illustration of how dramatically distance changes performance. It notes that a handheld system can deactivate an average bacterium in 17 seconds at a 4-inch distance with a dose of 2.80 mJ/cm², while 15 feet requires 28 minutes to reach the same 50 mJ/cm² target dose in that example. That gap is why consumer expectations often collide with physics.
What professionals measure
Professional remediation teams don't guess their way through this. They account for:
- Lamp output. The unit's actual germicidal intensity.
- Surface geometry. Flat counters behave differently than chair rails, vents, and fabric seams.
- Exposure duration. The cycle has to match the target and the space.
- Obstructions. Furniture, equipment, bed frames, and cabinetry all create loss zones.
If the dose isn't measured or validated, the disinfection claim is weaker than most people think.
This is the technical gap between a marketed UV product and a defensible remediation protocol.
Limitations UV Disinfection Is Not a Magic Bullet
The biggest misunderstanding around UV is the belief that it reaches everywhere. It doesn't. UV is line-of-sight technology. If the light can't directly hit a surface, that surface may not receive effective disinfection.
That one fact explains most real-world failures.

Shadowing is the hidden weakness
Take a simple living room. The top cushion of a sofa may be illuminated. The underside of the armrest isn't. The narrow gap between the sofa and the wall isn't. The lower edge of a coffee table leg creates a shadow line. A remote control in a tray can shield its own underside.
That is what professionals mean by shadowing.
The problem gets worse in spaces filled with equipment, textiles, cords, shelving, or irregular surfaces. In a clinic or industrial setting, there may be dozens of hidden surfaces that a static UV unit will never touch directly.
Dirt blocks light
UV also doesn't penetrate soil well. Dust, dried residues, body fluids, and grime can shield microorganisms from exposure. That is why manual precleaning isn't optional.
If you're weighing cleaning terminology, the difference between sanitizing, disinfecting, and sterilizing matters here because UV is often discussed as if it automatically "sterilizes" a room. In practice, the outcome depends on preparation, validated dose, and environmental complexity.
Lab performance and field performance are different
According to the systematic review in PMC, laboratory conditions often yield 2- to 6-log₁₀ reductions, while real-world surface disinfection combined with manual precleaning typically achieves only 1- to 2-log₁₀ reductions. The same review concludes that UV-C is a supplementary method rather than a stand-alone replacement for chemical cleaning in complex biohazard scenarios.
That finding lines up with what experienced remediation crews already know. Controlled test coupons are not cluttered apartments, active patient rooms, locker rooms, or contaminated vehicles.
Where marketing claims often break down
Many home devices are sold as if UV alone is enough. The practical problems usually fall into a few categories:
- Weak output. The lamp doesn't deliver enough germicidal energy.
- Poor positioning. The user treats open surfaces and misses shadowed ones.
- Short cycles. The unit runs for convenience, not for validated dose.
- Dirty surfaces. Organic matter remains and blocks exposure.
A UV cycle can create confidence without creating full coverage. That's the risk managers need to guard against.
Safety Protocols and Regulatory Standards
A room can look clean, smell clean, and still be unsafe to enter during or after a UV cycle. That disconnect causes problems. In biohazard work, UV adds a second hazard to the first one. You are controlling infectious material and a radiation source at the same time.

UV-C damages nucleic acids in microbes. Human eyes and skin are built from vulnerable cells too, so they can be injured by the same energy if exposure is not controlled. Ozone can also become part of the risk picture with some UV wavelengths and lamp designs, which means air quality has to be considered along with surface treatment.
That is why professional UV use is built around engineering controls first, not just operator caution. The room is cleared. Doors are secured. Warning signage is posted. Remote activation, timed cycles, shutoffs, and re-entry procedures are set before the lamp turns on, not improvised halfway through the job.
The CDC guidance on ultraviolet radiation explains that occupational exposure can injure the eyes and skin, and it frames UV as a workplace hazard that requires control measures. That is the right lens for facility managers. A UV device should be treated less like a household gadget and more like restricted equipment with a written operating procedure.
Why open-room use needs controlled setup
Handheld tools, upper-room fixtures, and whole-room units do not carry the same risk profile. A handheld lamp puts safety in the operator's hands second by second. A room unit shifts the problem to access control, placement, validation, and safe re-entry. In both cases, the rule is the same. No one should be exposed because a cycle was started casually or a device was trusted without confirming how it is meant to be used.
Worker protection also has to account for the original contamination. UV does not replace splash risk, inhalation risk, sharps risk, or contact risk. Teams reviewing procedures should use the baseline personal protective equipment standards for hazardous cleanup work alongside the UV-specific controls for the device in use.
In facilities that are modifying a room for fixed UV equipment, electrical layout and fixture selection matter as much as the lamp itself. A qualified commercial lighting contractor can help evaluate placement, power, shielding, and code-related installation issues before the system is put into service.
Regulatory expectations are narrower than marketing claims
A common mistake is assuming germicidal light automatically satisfies disinfection obligations. It does not. OSHA's Bloodborne Pathogens Standard still requires employers to use appropriate engineering controls, work practices, training, and suitable decontamination procedures for the hazard present. EPA regulation also applies to many antimicrobial product claims, which means a vendor's promise is not the same as a validated, compliant method.
For healthcare environments, the ASHRAE position document on infectious aerosols is useful because it places UV in the larger infection-control system rather than treating it as a stand-alone answer. That framing matches field reality. UV may support risk reduction, but it has to be paired with room preparation, appropriate cleaning chemistry where required, occupancy controls, and documented procedures.
For readers who want a quick visual overview of UV safety concerns and handling context, this short explainer is useful:
What trained operators actually do
Teams that use UV well build safeguards around both the people and the process:
- Restrict access with door controls, signage, and clear chain-of-custody for the treatment area.
- Match the device to the task so the wavelength, mounting style, exposure pattern, and cycle design fit the room and contamination scenario.
- Follow manufacturer instructions and site SOPs for placement, timing, warm-up, cooldown, and re-entry.
- Verify safe use conditions including shielding, sensor function, and whether the area is occupied or unoccupied during operation.
- Document the treatment so there is a record of who operated the unit, under what conditions, and with what precautions.
A strong program treats UV as a controlled tool inside a larger remediation plan. That is where it delivers value, and where it stays defensible under scrutiny.
Integrating UV into a Remediation Plan
A room can look clean, smell clean, and still fail a real remediation standard. That is usually where facility managers get pulled off course by UV marketing. The device is presented as the answer, when in practice it belongs later in the sequence, after the conditions for success have been created.
A useful comparison is floor waxing. You would not wax over dirt and call the floor restored. UV works the same way. It can support the final outcome, but it cannot compensate for soil left on surfaces, missed debris, blocked line of sight, or poor room preparation.
The workflow professionals follow
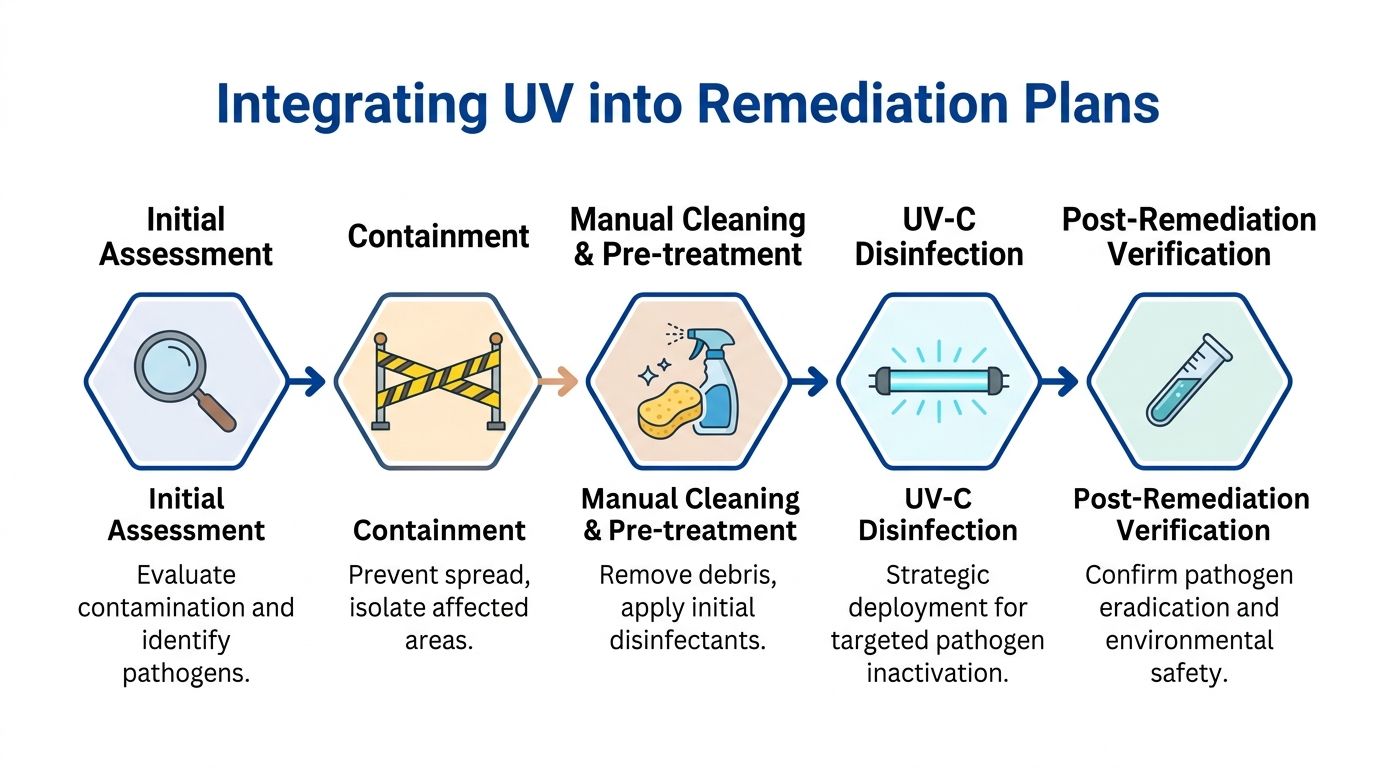
A defensible remediation plan usually moves through five stages:
Assessment and hazard mapping
The crew identifies the contamination type, where material likely spread, which surfaces are porous or non-porous, and who may be exposed if the area is returned to service too soon.Containment and removal
Gross contamination is isolated and removed first. Waste handling follows the rules for packaging, transport, and disposal so the cleanup does not create a second exposure problem.Manual cleaning and chemical disinfection
Physical cleaning removes the material that can shield microbes from later treatment. Then the selected disinfectant is applied according to label directions and contact time.Targeted UV terminal treatment
UV is used only after the room has been cleaned and arranged so the light can reach the intended surfaces. In that role, it serves as a finishing step, not the main event.Post-remediation verification
The team records what was done, checks whether the area meets the site standard for re-entry, and documents any limits on what UV could or could not reach.
Facilities planning room-based UV systems often need help beyond infection control. Power supply, mounting location, shielding, and fixture layout affect whether the equipment can be used safely and consistently. In those cases, a qualified commercial lighting contractor can support the electrical side of the installation.
Where UV fits in the real world
The strongest use case is controlled terminal treatment after hands-on cleaning is complete. Hospitals, clinics, laboratories, and biohazard crews use UV in that narrow role because it can add another layer on exposed surfaces in a prepared space.
That point matters because the gap between brochure language and field performance is usually a setup problem. A cluttered room, an uncleaned spill, a shadowed corner, or a rushed cycle can turn an expensive UV unit into little more than a bright box. Good planning closes that gap.
In practical biohazard work, UV makes the most sense after trauma cleanup, medical contamination, isolation-room turnover, or other events where the area has already gone through removal, cleaning, and surface disinfection. It is one layer in a stack of controls.
Why specialized equipment matters
The machine itself is only part of the system. Output, wavelength, room geometry, stand height, sensor placement, cycle length, and operator judgment all affect whether the treatment has a fair chance to work.
That is why crews using specialized biohazard cleanup equipment need more than product familiarity. They need to know when to reposition the unit, when another method should take priority, and when UV should be left out because the environment is too complex or the risk of misuse is too high.
Good remediation plans use overlapping controls so one weak point does not decide the whole outcome.
That is the professional view of UV. Useful, technical, and limited by real-world conditions.
When to Trust Professionals for Disinfection
Some situations don't leave room for trial and error. If the space involves blood, bodily fluids, trauma, infectious disease concerns, healthcare occupancy, vulnerable residents, or workplace exposure issues, professional help isn't a luxury. It's the correct risk decision.
A good rule is simple. If you need to prove a space is safe, not just hope it is, you need trained remediation professionals. UV light disinfection can support that outcome, but only when the crew understands dose, shadowing, cleaning prerequisites, worker safety, and regulatory compliance.
Signs the job is beyond consumer tools
- Biohazard involvement means disposal, PPE, and decontamination rules apply.
- Shared or sensitive occupancy such as clinics, schools, offices, and multifamily housing raises the consequences of an incomplete cleaning job.
- Complex room geometry increases the chance that UV alone will miss critical areas.
- Need for documentation usually means the work has to stand up to insurance, management, or regulatory scrutiny.
Families and facility managers are often under pressure to restore normal use quickly. Speed matters, but unsupported speed creates risk. The safer path is a documented remediation plan carried out by people who know where UV fits, where it fails, and how to protect everyone involved.
When disinfection has to be credible, measured, and compliant, choose a provider that treats the situation with technical discipline and human sensitivity.
When you need a team that can handle trauma scenes, infectious contamination, unattended death cleanup, industrial hazards, and compliant remediation with compassion, 360 Hazardous Cleanup provides experienced, around-the-clock support. They help families, facility managers, healthcare organizations, property owners, and insurers manage high-stress situations with safe procedures, clear communication, and respect for privacy.
