You're usually reading about hospital disinfection services when something has already tightened the margin for error. Bed turnover is behind schedule. A unit has a pathogen-specific concern. Survey readiness is hanging over the week. Someone wants a faster room release, someone else wants stricter controls, and both expect zero compromise on patient safety.
That describes the operating environment. In hospitals, disinfection isn't a housekeeping afterthought. It sits inside infection prevention, staffing, patient throughput, regulatory exposure, and public trust. A room can look clean and still fail the standard that counts, which is whether the process reduced risk in a reliable, repeatable, documented way.
Facility managers know this better than most. The hard part usually isn't identifying that disinfection matters. It's building a program that works across shifts, room types, surface types, and changing clinical demands without drifting into guesswork or wasted effort.
The Critical Importance of Hospital Disinfection
At 6:40 a.m., a discharged patient room looks ready. Bed rails are dry. Floors appear clean. The next admission is waiting. But if high-touch surfaces were missed, the disinfectant sat for too little contact time, or the wrong product was used on the wrong material, the hospital has not reduced risk. It has only created the appearance of control.
That distinction matters to facility managers because disinfection affects more than environmental appearance. It affects exposure control, room availability, survey readiness, incident response, and the hospital's ability to show that its process holds up under pressure. A strong program is not defined by how fast a room turns. It is defined by whether staff can execute the same standard correctly across units, shifts, and patient conditions.
Hospitals run into trouble when disinfection is treated as a supply choice instead of an operating system. Product selection matters, but performance usually breaks down elsewhere. Training drifts. Room categories get oversimplified. Supervisors chase throughput without checking technique. Documentation exists, but it does not prove the work was done in a repeatable way.
Three management concerns sit at the center of this issue:
- Risk reduction: Shared surfaces, mobile equipment, and touchpoints can contribute to transmission when protocols are inconsistent or poorly matched to the care setting.
- Operational performance: Delays, rework, and precautionary holds affect bed flow, staff coordination, and daily throughput.
- Defensible compliance: During a complaint, survey, or infection review, “the room looked clean” is not a defensible standard.
The trade-off is real. Pushing for shorter turnover times without validating execution creates avoidable risk. Building a process so complex that staff cannot follow it consistently creates a different failure. Good hospital disinfection programs are designed for actual hospital conditions, not ideal ones. They account for staffing variation, different surface materials, isolation requirements, and the fact that an emergency department bay does not present the same contamination profile as a med-surg room or behavioral health space.
Pathogen-specific pressure makes that gap visible fast. For a practical example, 360 Hazardous Cleanup's overview of MRSA in hospitals and the critical cleanup process shows why surface control depends on disciplined execution, verified steps, and clear accountability.
Poor programs tend to fail in familiar ways:
- One workflow is applied everywhere: The same sequence, chemistry, and timing are used across rooms with different risks and surfaces.
- Speed becomes the only scorecard: Rooms are released quickly, but no one verifies whether high-touch disinfection was completed correctly.
- EVS is left outside the control structure: Staff carry infection-control responsibilities without being fully integrated into training, escalation, and audit processes.
- Cross-contamination controls are weak: Tool handling, cart setup, and sequencing break down in ways any operations manager would recognize from other hygiene-sensitive environments, including maintaining food safety in kitchens.
Facility managers do not need a vendor who promises to disinfect more thoroughly. They need a partner and an internal program that can support protocol discipline, verification, escalation, and documentation. That is the difference between routine cleaning activity and a disinfection system the hospital can trust.
The Critical Difference Between Cleaning Disinfecting and Sanitizing
People often use these terms interchangeably. In a hospital, that creates trouble fast.
Cleaning removes soil, organic matter, dust, and residues from a surface. Sanitizing lowers the microbial load to a level considered acceptable in some settings. Disinfecting uses an appropriate chemical process to inactivate or eliminate specified pathogens on a clean surface. Those aren't branding variations. They are different outcomes.

Think of surface care like site preparation
A simple analogy helps. If a floor has visible debris, body fluid residue, adhesive buildup, and dust, applying disinfectant immediately is like painting over grease and expecting the finish to bond. The chemistry may be correct, but the surface condition blocks performance.
That's why effective hospital disinfection services follow a sequence:
- Remove visible soil and organic load
- Apply the correct disinfectant to the correct surface
- Allow the required dwell or contact time
- Use a method that matches the contamination risk
If step one is skipped, step two often underperforms. That's true in healthcare, food production, and any environment where contamination control matters. The logic behind surface prep is similar to the way professionals approach maintaining food safety in kitchens, where cross-contamination control depends on sequence, separation, and method rather than simple appearance.
Why sanitizing isn't enough in clinical spaces
Sanitizing has a role in many commercial environments. Hospitals are different because surfaces may be exposed to pathogens that demand a higher level of control, especially in patient-care areas, isolation settings, and discharge cleaning.
A “deep clean” can still miss the mark if it focuses on effort rather than outcome. More wiping, more fragrance, or more product doesn't automatically mean better disinfection. The question is whether staff removed interfering soil, used the right chemistry, and treated the right surfaces in the right order.
A plain explanation of that distinction is helpful when teams are mixing up scopes of work. 360 Hazardous Cleanup addresses this directly in its guide to biohazard vs standard cleaning, which is especially relevant when bodily fluids, isolation cleaning, or infectious disease response enters the picture.
The mistake that causes repeated failures
The most common field error is simple. Staff disinfect dirt.
That usually happens because:
- Turnover pressure shortens pre-cleaning
- The wrong cloth or wipe is used for the amount of soil present
- Contact time is ignored once the surface “looks done”
- Teams treat all touchpoints as equal when they aren't
A surface can be visually improved and microbiologically unmanaged at the same time.
Facility managers don't need staff to memorize textbook definitions. They need crews who understand the chain of cause and effect. Cleaning prepares the surface. Disinfecting controls the hazard. Sanitizing, in many hospital applications, doesn't go far enough.
A Facility Manager's Guide to Disinfection Technologies
Hospitals now have more disinfection technology options than ever. That sounds like progress, but it also creates a procurement problem. Vendors often present tools as if one platform can solve every contamination scenario. It can't.
The better way to evaluate hospital disinfection services is to think in terms of a toolkit. Each method has an operating window, a best-fit use case, and failure points that show up quickly when the wrong tool is forced into the wrong setting.
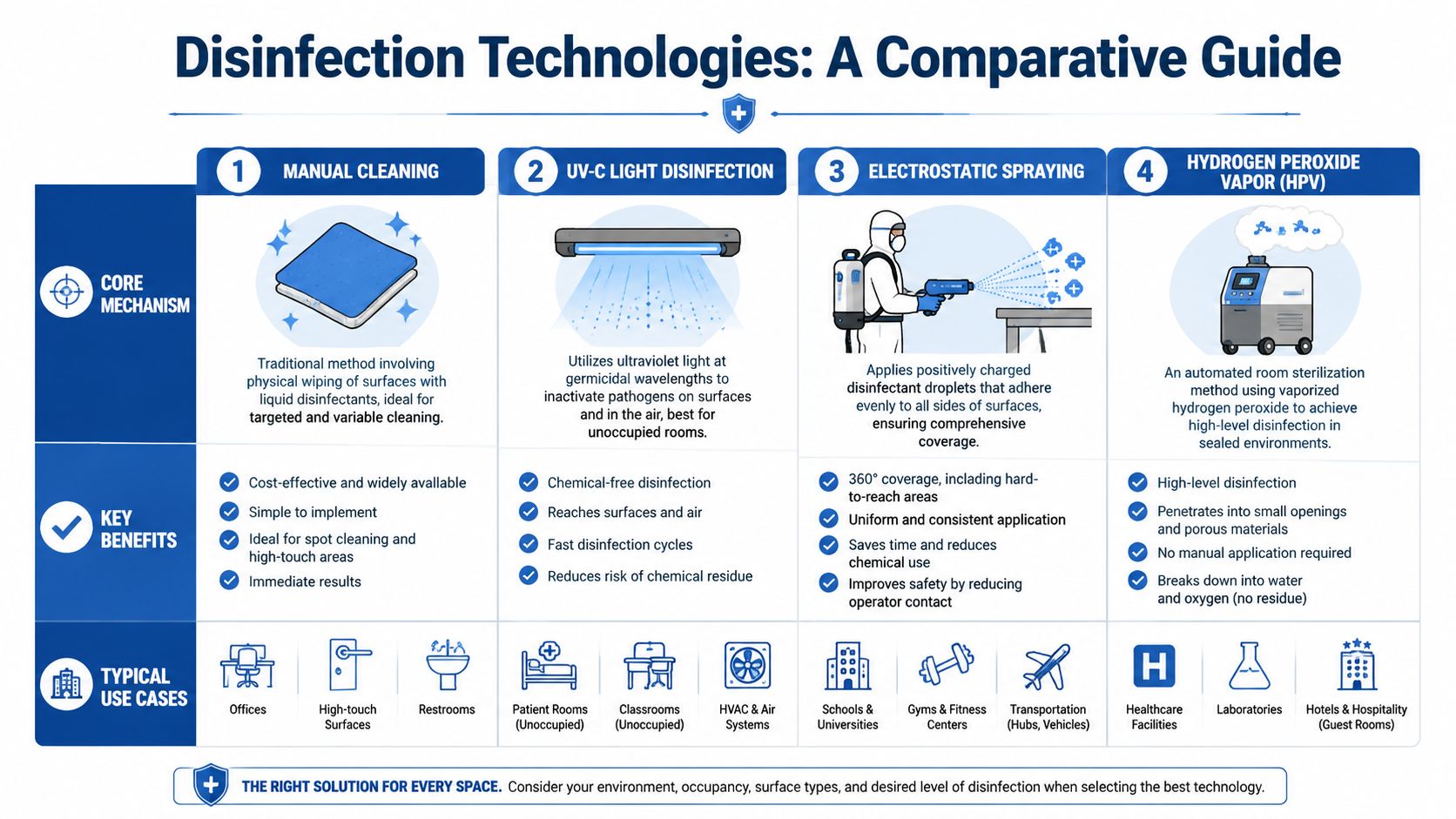
The comparison that matters on the floor
| Method | Best use | Main strength | Main limitation |
|---|---|---|---|
| Manual wiping and liquid application | Daily cleaning, targeted high-touch work, visible soil removal | Direct control over surfaces and sequence | Quality depends heavily on technique |
| Terminal cleaning | Post-discharge or isolation-room reset | Comprehensive room-by-room decontamination workflow | Slower, labor-intensive, easy to shortcut under pressure |
| UV-C systems | Added layer in unoccupied rooms after manual prep | No-touch support for exposed surfaces | Shadows and line-of-sight issues limit coverage |
| Electrostatic spraying | Complex geometries and broad surface coating | Even distribution across irregular surfaces | Not a substitute for physical soil removal |
| Hydrogen peroxide vapor or similar room systems | High-concern spaces requiring controlled whole-room treatment | Strong room-wide decontamination potential in sealed environments | Requires vacancy, planning, and strict process control |
Manual work still carries the program
Many hospitals get distracted by automation and forget the foundation. Manual cleaning and wiping still do the heavy lifting because someone has to remove soil, address touchpoints deliberately, and work around real-world clutter, equipment cords, bed rails, monitors, and soft goods.
That's also where disinfectant selection becomes highly technical. Product choice should be pathogen-specific and surface-specific. For example, EPA-registered sporicidal products are required for Clostridioides difficile terminal cleaning, while standard quaternary ammonium compounds aren't sufficient against spores. The same source notes that hand-contact sites with bioburden at or above 5 cfu/cm² suggest increased infection risk, which supports matching product, frequency, and contact time to actual risk rather than using more chemistry, as explained in this review of deep cleaning versus regular hospital cleaning.
Soft and porous materials complicate the picture further. Upholstered seating, privacy curtains, and foam-covered surfaces often can't be reliably disinfected with wipes alone. In those cases, laundering, steam treatment, or replacement may be the safer operational choice.
Where no-touch tools help and where they don't
UV-C, electrostatic sprayers, and vapor-based room systems can add value, especially in post-discharge disinfection, outbreak response, or high-concern rooms that need standardized treatment. But each comes with conditions.
- UV-C works best after proper manual prep: Dust, residue, and shadowed surfaces reduce effectiveness.
- Electrostatic systems improve coating uniformity: They don't solve poor chemistry selection or skipped pre-cleaning.
- Hydrogen peroxide vapor systems demand controlled conditions: Room vacancy, sealing, ventilation planning, and re-entry controls matter.
For facilities weighing these options, it helps to understand how modern tools fit into broader decontamination strategy. This overview of how decontamination technology has advanced in the last 5 years is useful context when vendors start promising speed without discussing operating constraints.
One more point gets overlooked. Some technologies affect workflow beyond the room itself, especially when air handling, room downtime, or reoccupancy timing enters the discussion. Facility teams comparing environmental controls may also find value in Wilcox Door Service Inc. air quality information when considering how airborne management and surface disinfection intersect in occupied buildings.
Don't buy a machine. Buy a use case, a protocol, and a validation plan.
A practical selection lens
When reviewing a technology proposal, ask four direct questions:
- What problem is this solving? Routine turnover, outbreak containment, isolation discharge, or odor and residue control are not the same scope.
- What must happen before deployment? If the answer ignores pre-cleaning, the proposal is incomplete.
- What surfaces or room conditions limit performance? Every method has blind spots.
- How will the hospital verify results? A technology claim without a verification process is just marketing.
Used correctly, advanced tools can strengthen a hospital program. Used as a substitute for process discipline, they usually create expensive confidence.
Building Compliant and Effective Disinfection Protocols
At 2:15 a.m., the ED is still full, an isolation discharge just hit the queue, and the night supervisor is covering a callout. That is when a disinfection protocol proves its value. If the process only works during a survey week, with full staffing and ideal room conditions, it is not a dependable control.
Hospitals need protocols that hold up under pressure. That means clear room-specific instructions, realistic task times, defined escalation paths, and documented oversight. As noted earlier, federal infection-control guidance treats environmental cleaning as a managed system tied to training, staffing, and risk reduction. Facility managers should approach protocol design the same way. Build it like an operational control, validate it in real conditions, and revise it when the field reality changes.
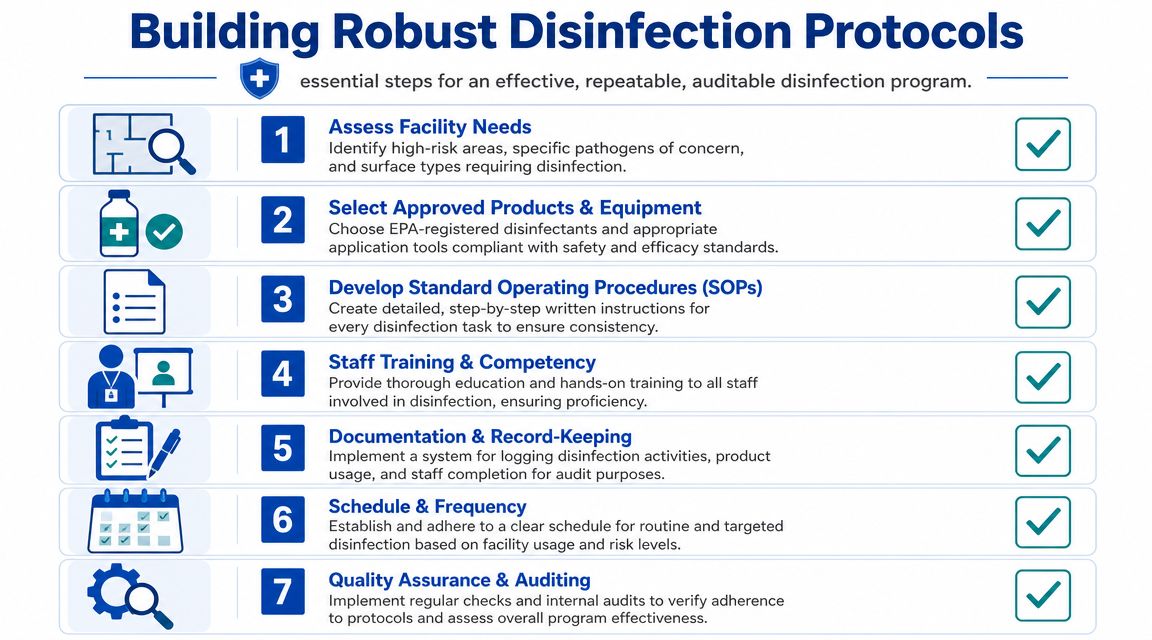
Start with room type, not product catalog
A compliant program starts with risk classification. Patient rooms, airborne isolation rooms, procedure spaces, public bathrooms, waiting areas, and shared transport equipment do not carry the same exposure profile or turnover pressure. They should not share the same SOP.
A workable protocol usually defines:
- Room categories and triggers: Staff know which SOP applies before entering the space and when a condition changes the process.
- Surface-level instructions: Bed rails, call buttons, monitors, grab bars, bathroom fixtures, keyboards, pumps, and shared devices get explicit treatment steps.
- Approved chemistry by surface and setting: Teams know what product to use, where it is approved, what contact time is required, and where material compatibility is a concern.
- Escalation events: Isolation discharge, blood or bodily fluid contamination, suspected spore-forming organisms, and terminal cleaning events shift the workflow immediately.
This is less about housekeeping preference and more about process control. If the protocol leaves room for interpretation, variation will show up first on the highest-risk surfaces.
Minimum cleaning time is a capacity decision
Cleaning time is one of the quickest ways to see whether leadership expectations match labor reality. I have seen well-written SOPs fail because the room assignment model assumed ideal turnover conditions and ignored clutter, delayed restocking, or the extra minutes needed to meet label contact time.
If a room cannot be cleaned to standard in the time allowed, the problem is not staff attitude. The problem is protocol design, staffing, or both.
A reliable program accounts for five variables:
- Observed task duration by trained staff
- Room complexity, equipment density, and clutter
- Shift-to-shift staffing variation
- Supply access and refill reliability
- Time needed for correct disinfectant contact time
One practical rule applies here. If the protocol only succeeds when nothing interrupts the sequence, it is too fragile for a hospital.
Hospitals also need the worker-safety side aligned with the infection-control side. Blood and bodily fluid response, PPE selection, waste handling, and exposure documentation all intersect with disinfection work. 360 Hazardous Cleanup's guide to OSHA and biohazard cleanup compliance and safety standards is a useful reference when reviewing whether environmental protocols also meet worker-protection requirements.
The best SOPs remove guesswork
“Disinfect all high-touch surfaces” is not an instruction. It is a placeholder.
A usable SOP tells the technician what order to work in, which wipe or cloth system to use, how to handle porous or damaged materials, what to do when equipment blocks access, and how completion gets documented. It also addresses common failure points before they become routine shortcuts.
In practice, drift usually follows a familiar pattern:
- Staff change the sequence to save steps
- Obstructed surfaces get skipped
- Products are substituted without compatibility review
- Night and weekend teams inherit informal shortcuts
That is why competency cannot be treated as a one-time orientation item. Staff need initial instruction, observed demonstration, refresher training, and direct correction when process drift appears. The strongest environmental services teams are managed with the same discipline hospitals expect from other high-consequence workflows.
Audits should improve execution
Audit programs work best when they identify system weakness, not just individual misses. A supervisor should be able to observe room execution, compare it to the SOP, spot repeated breakdowns, and determine whether the root cause is training, staffing, supply flow, room condition, or an unrealistic protocol step.
That is the difference between a cleaning checklist and a compliance system. The goal is not confined to asking whether a room was serviced. The goal is to make correct execution repeatable, defensible, and measurable across every shift.
The Science of Verification Proving Disinfection Efficacy
Many hospitals still rely too heavily on visual inspection. That standard is too weak for healthcare.
A room can pass the eye test and still leave behind residue, missed touchpoints, or an inconsistent application pattern. The primary concern isn't whether the floor shines or the sink looks polished. It's whether the process reduced contamination risk on the surfaces most likely to matter.
Visible cleanliness is not proof
A 2023 review of hospital cleaning points to an issue facility leaders already feel on the ground. Visible cleanliness is only part of the issue, environmental reservoirs can contribute to healthcare-associated infections, and one of the most important unanswered operational questions is how to validate whether a disinfection program effectively reduced risk for a specific unit and turnover pattern, as discussed in Hospital cleaning past present and future.
That matters even more when hospitals add UV-C, robotics, electrostatic spraying, or continuous disinfection technologies. The tool itself doesn't prove the outcome.
What verification should look like
In practice, verification should combine routine oversight with targeted measurement. The exact mix will vary by unit, risk profile, and event type, but a serious program usually includes several layers.
- Defined critical surfaces: Bed rails, overbed tables, bathroom fixtures, call controls, and shared device touchpoints should be identified in advance.
- Process observation: Supervisors should watch whether staff follow the SOP in the field, not just sign off afterward.
- Surface testing where appropriate: ATP monitoring can provide a rapid indicator of residual organic contamination on selected surfaces.
- Targeted culture-based investigation in higher concern scenarios: During an outbreak review or a recurring problem, more specific microbiological assessment may be warranted.
- Corrective action tracking: Verification has value only if missed steps change future behavior.
If a contractor's report only says “area disinfected,” you haven't received evidence. You've received a statement.
Ask for evidence that changes decisions
Facility managers should expect documentation that helps them manage the program, not just close the ticket. Useful reporting answers practical questions:
| Question | What useful verification provides |
|---|---|
| Did staff follow the protocol? | Observation records, task completion logic, or audit notes |
| Were critical surfaces addressed? | Surface-specific checklists or verification targets |
| Did the process improve cleanliness? | Before-and-after measurement where that method is part of the program |
| What needs adjustment? | A clear record of recurring misses, retraining needs, or protocol gaps |
Verification also protects the hospital from false confidence. If one unit repeatedly shows weak post-cleaning results, the solution may not be “buy more technology.” It may be poor workflow design, unrealistic room-release timing, supply problems, or inconsistent training.
That's why quantitative and observational checks matter. They turn disinfection from a visual ritual into a monitored control process.
How to Choose a Hospital Disinfection Partner You Can Trust
The wrong disinfection partner creates work for your team. The right one removes uncertainty.
Most providers can describe products, PPE, and “deep cleaning.” Far fewer can explain how they document chain of activity, train crews for clinical environments, handle regulated waste, support outbreak response, and align with hospital compliance expectations without disrupting operations.
Evaluate the partner like a risk vendor
A hospital shouldn't hire disinfection support the way it hires routine janitorial overflow. The exposure is different. Start with the questions that affect liability, documentation, and operational control.
Look for a partner that can clearly address:
- Training and competency: Staff should be trained for healthcare and biohazard conditions, not just commercial cleaning.
- OSHA-aware field execution: The provider should understand worker protection, PPE discipline, and hazardous exposure controls.
- Documentation standards: You want service records that hold up internally and, if needed, externally.
- Emergency response capability: Timing matters when a room, unit, or incident can't wait for standard scheduling.
- Discretion and coordination: In occupied facilities, contractors need to move professionally around patients, staff, and sensitive incidents.
A practical buyer's checklist appears in 360 Hazardous Cleanup's article on what to consider when choosing a biohazard cleanup company. The questions there are especially useful when a hospital needs more than standard EVS support.
Ask where advanced disinfection is actually justified
A strong partner won't push the same treatment everywhere. That conversation matters because one of the major strategic questions in healthcare cleaning is which zones merit advanced disinfection versus routine cleaning, especially when facilities are trying to balance infection control, worker exposure, material compatibility, and sustainability as automated and persistent technologies become more common, as discussed in this hospital cleaning services overview.
That means your prospective provider should be willing to say:
- some spaces need enhanced controls,
- some need disciplined routine disinfection,
- some need careful product restrictions because of surfaces or equipment,
- and some problems are better solved by workflow correction than by adding more chemistry.
That kind of restraint is a good sign. It shows the company understands consequence, not just equipment.
What a useful partner discussion sounds like
A productive scoping call usually includes questions such as:
- Which pathogens or contamination scenarios are driving concern right now?
- What room types are involved, and are any porous or sensitive materials present?
- What proof of completion and proof of effectiveness does the hospital expect?
- Will work occur in occupied, semi-occupied, or vacant spaces?
- Who owns post-service signoff and escalation if conditions change?
One factual option in this category is 360 Hazardous Cleanup, which provides infectious-disease cleanup and professional hazmat disinfection services for environments that require trained biohazard handling and compliant remediation support. That sort of capability is most relevant when a hospital needs specialized response beyond routine environmental services.
The best partner isn't the one with the longest equipment list. It's the one that can explain when not to use a tool, how to document the work, and how to protect your staff and your facility if conditions change mid-job.
Price matters less than controllability
Every facility has a budget. But hospital disinfection is one of those categories where low-bid thinking can lead to a subtle increase in total risk.
A cheaper vendor can cost more if they:
- create rework,
- damage materials with the wrong chemistry,
- fail to document the scope,
- expose the hospital to worker-safety issues,
- or disrupt throughput because they don't understand healthcare operations.
The better buying question is simple. Will this partner help your hospital run a more controlled, auditable, lower-risk environment?
If the answer isn't clear, keep looking.
Partnering for a Safer Healthcare Environment
Hospital disinfection services work when they're treated as a disciplined control system. Not a spray-and-wipe routine. Not a technology showcase. And not a generic service line borrowed from commercial cleaning.
Facility managers need programs that match the room, the pathogen concern, the surface type, and the challenges of staffing and turnover. They also need proof. That means room-specific protocols, trained personnel, measured execution, and verification that goes beyond appearance.
The right disinfection partner supports all of that. They help the hospital reduce risk, protect staff, document performance, and respond professionally when conditions are sensitive or time-critical. That's the standard healthcare environments deserve.
If your facility needs a practical review of current disinfection workflows, incident response readiness, or specialized infectious-disease cleanup support, 360 Hazardous Cleanup can help assess the risks, clarify the compliance demands, and support a safer, more defensible operating environment.
