
A positive MRSA result tends to land with two kinds of pressure at once. Clinical staff need a clear isolation plan immediately, and whoever oversees the building starts thinking about exposure, cleaning, family concerns, staffing strain, and liability. In long-term care, clinics, behavioral health settings, and even private homes, that pressure is justified.
MRSA isolation precautions matter because MRSA isn't just a treatment issue. It's an environmental and operational issue. People touch bed rails, call buttons, bathroom fixtures, keyboards, carts, wheelchairs, linens, door hardware, and shared equipment long before anyone sees a problem. If the response is delayed, inconsistent, or handed off to people who weren't trained for infectious contamination, the room can become the source of the next incident.
The response has to be calm and disciplined. That means knowing when isolation is warranted, how PPE and hand hygiene should be performed, where routine housekeeping ends, and when certified biohazard remediation becomes the safer and more compliant choice.
Understanding the Urgency of MRSA Precautions
The call usually starts the same way. A nurse manager, administrator, property manager, or family member has just been told someone in the building is MRSA-positive. The first question is often practical, not academic. What do we do right now, and how much of this can our staff safely handle?
MRSA stands for methicillin-resistant Staphylococcus aureus. What makes it urgent isn't only the organism itself. It's the combination of contact spread, vulnerable occupants, and the false sense of security that can come from doing a little cleaning and assuming the problem is contained.

In the United States, the CDC estimates MRSA causes over 70,000 severe infections and 9,000 deaths annually, and progress on hospital-onset MRSA bacteremia has stalled, which is why infection control still demands close attention across settings, not only hospitals (MRSA burden and precaution context in this review).
Why a single positive result changes the room
Once MRSA is confirmed or strongly suspected, the room can't be treated like ordinary occupied space. Staff movement, supply flow, linen handling, and visitor access all need structure. In a hospital or nursing facility, that affects care delivery. In a residence or commercial property, it affects who can safely enter, what can leave the room, and what surfaces may now require more than standard janitorial attention.
A lot of people still assume the major risk is dramatic contamination. In practice, the harder problem is routine contact. A gloved hand touches a contaminated rail, then a chart, then a cart handle. A staff member adjusts a gown incorrectly. A visitor sits in a chair that wasn't cleaned properly. Those ordinary actions are how isolated mistakes become facility-wide headaches.
MRSA control isn't built on panic. It's built on repeatable habits, clear room rules, and disciplined cleaning boundaries.
The stakes for facilities and families
For facility leaders, the stakes include outbreak control, staff confidence, documentation, and defensible compliance decisions. For families, the stakes are more personal. They want to know whether their loved one is safe, whether the room is safe, and whether they can trust what "cleaned" really means.
That distinction matters. A room can look clean and still be high risk.
If you're dealing with MRSA in a healthcare environment, this overview of MRSA in hospitals and the cleanup process is a useful companion to isolation planning because it frames the problem as both infection control and contamination control.
When to Implement MRSA Isolation Precautions
Waiting for certainty is one of the most common response failures. In real operations, you don't start precautions only when the paperwork feels complete. You start when the risk picture says delay could expose staff, residents, patients, or visitors.

The most common triggers
Start MRSA isolation precautions when any of these conditions are present:
- Confirmed MRSA status from a lab result, transfer paperwork, or documented medical history.
- Known prior colonization or infection when the person is re-admitted or transferred into a shared-care environment.
- Draining wounds or skin lesions that can't be fully contained and covered.
- High-risk transfers from facilities or units where MRSA is a known concern.
- Clinical uncertainty with active exposure potential, especially if staff will have close physical contact or handle contaminated items before final confirmation.
In outpatient and community-adjacent settings, the decision can be more nuanced. A person in a private office with no direct care needs isn't managed the same way as a resident in memory care with skin breakdown and frequent hands-on assistance. The point is to match the precautions to the contact risk, not to use one script for every environment.
For broader facility planning, MRSA Prevention in High-Traffic Facilities is a helpful reference because it pushes managers to think beyond the patient room and consider traffic patterns, shared surfaces, and operational chokepoints.
The first communication steps
Once precautions begin, communication can't be vague. Staff need to know what the room status is, what PPE is required, what equipment is dedicated to the room, and who is responsible for cleaning and waste flow.
Use a simple communication chain:
- Notify direct care staff first so no one enters unprotected.
- Alert environmental services or housekeeping with room-specific instructions.
- Inform supervisory personnel so staffing and documentation stay aligned.
- Brief family and approved visitors in plain language.
- Flag transport and receiving departments if the person is leaving the room for tests, treatment, or transfer.
People comply better when instructions are concrete. "Use precautions" is too loose. "Gown and gloves before room entry, dedicated equipment only, bag waste inside the room" is workable.
Practical rule: If a temporary worker, float nurse, contractor, or family member could misunderstand the sign, the sign isn't clear enough.
What the room sign should do
An effective sign should answer the questions a person has before they touch the doorknob. It doesn't need clinical jargon. It needs clarity.
A good MRSA isolation sign should identify:
- Room status such as contact precautions
- Required PPE before entry
- Hand hygiene requirement
- Instructions for dedicated or disposable equipment
- Visitor direction, including who to contact with questions
- Transport note if movement outside the room requires additional steps
Avoid overloading the sign with policy text. The detailed procedure belongs in staff training materials. The sign is a stop signal and action prompt.
A decision point managers often miss
A positive room isn't only a nursing issue. It is also a facilities issue. Shared bathrooms, linen routes, EVS staffing, and after-hours coverage need immediate review. If the space later becomes vacant after discharge, death, or transfer, the response also changes. Daily room precautions and terminal remediation are not the same task, and treating them as interchangeable is where many organizations create avoidable risk.
The Core Protocol for PPE and Hand Hygiene
Most MRSA transmission failures don't happen because a facility lacked a policy. They happen because the policy broke down at the doorway, at the glove cuff, at the cart handle, or during PPE removal. Execution beats policy language every time.
A large VA long-term care study found that mandated contact precautions did not significantly reduce overall MRSA acquisition compared with standard precautions, but low compliance below 90% with PPE and hand hygiene in audited areas was linked to 20-30% higher transmission (VA long-term care findings in Clinical Infectious Diseases). That's the operational lesson. The protocol only works if people perform it correctly, consistently, and under real-world pressure.
What to wear and when
For standard MRSA contact precautions, the core PPE is:
- Gloves for room entry and contact with the person or contaminated surfaces
- Isolation gown when contact with the person, surfaces, linens, or equipment is likely
Masks and eye protection aren't automatically required for every MRSA room. They come into play when splash, spray, respiratory secretion exposure, or a procedure-specific hazard is present. Facilities often overcomplicate this point. Keep the baseline simple, then add face protection when the task warrants it.
A strong safety and PPE program helps reduce confusion because it standardizes training, stock placement, replacement, and competency checks across departments.
Donning sequence that actually works
Before entering the room, pause and check whether the needed supplies are within reach. Staff often contaminate themselves because they have to adjust PPE after opening the door or returning to the cart.
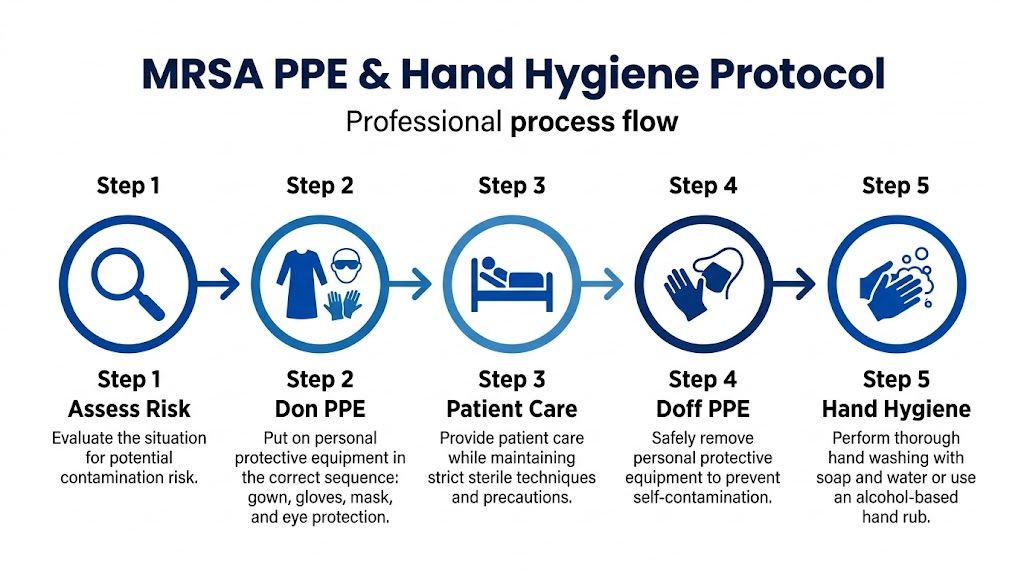
Use this sequence:
- Perform hand hygiene first.
- Put on the gown and tie or fasten it fully so clothing is covered.
- Apply the mask and eye protection if the task requires them.
- Put on gloves last, pulling them over the gown cuffs when appropriate.
The gown isn't a badge. It has to cover the body areas most likely to brush contaminated surfaces.
Many teams frequently lose consistency. Gloves go on too early. Phones get touched after donning. Staff adjust eyewear with contaminated gloves. The sequence matters because every out-of-order step creates another hand-to-face or hand-to-surface opportunity.
If your organization wants a broader operational view of field PPE expectations, proper PPE in biohazard cleanup gives useful context for why sequencing and removal discipline matter beyond bedside care.
A quick visual refresher helps reinforce the sequence:
During care inside the room
Once inside, PPE doesn't give permission to get sloppy. It buys a safer margin if the wearer maintains contact discipline.
Key habits include:
- Keep clean and dirty zones mentally separate. Don't touch your face, badge, or personal items.
- Use dedicated equipment when available. Shared cuffs, thermometers, and mobility aids create repeat exposure routes.
- Change gloves when the task changes. Dirty wound care and clean medication handling shouldn't happen on the same pair.
- Limit unnecessary surface contact. Leaning on the bed, setting supplies on counters, and resting gloved hands on carts all increase contamination spread.
Doffing without contaminating yourself
Removal is where experienced staff still make mistakes. They hurry, talk while removing gear, or grab the front of the gown.
A safer sequence is:
- Remove gloves carefully without snapping or skin contact.
- Remove gown by handling ties and the inside surfaces, then roll it inward.
- Exit according to facility protocol if room-based doffing is partial rather than complete.
- Remove eye protection and mask by straps or earpieces when used.
- Perform hand hygiene immediately.
Common mistake: Staff often think the dangerous moment is patient contact. In reality, the high-risk moment is often PPE removal.
Hand hygiene is the hinge point
Alcohol-based hand rub or soap and water must be available exactly where the workflow needs it. If dispensers are empty, far from the doorway, or hidden behind equipment, compliance drops. That's not a staff character problem. That's a systems problem.
Managers should watch for practical failure points such as poor dispenser placement, overfilled anterooms, missing glove sizes, and door hardware that forces recontact after hand hygiene. PPE training works best when it includes drills in the actual room setup, not just annual slides.
Environmental Controls Cleaning and Decontamination
The room itself can carry the problem forward long after staff feel the event is over. Bed rails, call buttons, overbed tables, bathroom fixtures, chair arms, remotes, privacy curtain edges, walkers, lift controls, and soft surfaces all need attention. MRSA isolation precautions fail when the environment is treated like a background issue.

Room placement and containment choices
Private rooms are preferred when available. If a private room isn't possible, cohorting may be used in clinical settings according to facility policy and medical oversight. The operational point is separation. Shared occupancy without disciplined controls turns every common touchpoint into a contamination management problem.
Environmental controls also include movement limits. Keep nonessential equipment out of the room. Dedicate what must stay. If an item has to leave, it should be cleaned and cleared under a documented process, not wiped casually in the hallway.
Daily cleaning during occupancy
Daily cleaning is necessary, but it has a narrow job. It reduces contamination pressure while the room is active. It does not substitute for full post-discharge or post-incident remediation.
During occupancy, teams should focus on:
- High-touch surfaces such as rails, bedside furniture, toilet handles, sink fixtures, light switches, and door hardware
- Shared care equipment if dedicated devices aren't possible
- Bathroom surfaces because splash and hand contact multiply risk
- Floor areas near the bed and bathroom where contaminated materials often move through footwear and carts
EPA-registered disinfectants should be used according to label instructions, including contact time. In practice, many cleaning failures come from rushing the dwell time or using the wrong product on the wrong surface.
A surface that was sprayed and wiped too quickly may look spotless and still not be disinfected as intended.
Where routine housekeeping reaches its limit
This is the line many facilities and families need explained clearly. Routine housekeeping supports infection control during occupancy. It is not the same as terminal decontamination after discharge, transfer, death, or a severe contamination event.
A standard janitorial approach often misses the hardest areas:
- Soft furnishings and porous materials
- Seams, crevices, and equipment undersides
- Privacy curtains and fabric partitions
- Stored items in drawers and cabinets
- Wheelchair grips, transfer boards, and mobility aids
- HVAC-adjacent dust reservoirs and overlooked vent surfaces
- Biofilm-prone zones around moisture and repeated touch
A 2025 study in Infection Control & Hospital Epidemiology found that 28% of MRSA outbreaks in long-term care facilities were traced to inadequate environmental cleanup after discharge, and viable bacteria were detected on 15% of high-touch surfaces 30 days after precautions were lifted (CDC MRSA infection control page cited in the provided brief). That finding captures the exact risk managers face when they assume the problem ended because the person left the room.
What terminal decontamination should involve
Once the person is discharged, relocated, or the event has otherwise ended, the space needs a different level of response. The objective shifts from daily reduction to verified clearance.
Professional post-incident decontamination may include:
Assessment of the contamination footprint
Not just the obvious room. Also bathrooms, adjacent touchpoints, transport paths, and shared equipment.Segregation of salvageable and non-salvageable contents
Some porous items can be treated. Others should be removed as regulated or precautionary waste depending on contamination and policy.Use of EPA-registered disinfectants with correct dwell times
Product selection matters. So does compatibility with the material being treated.Detailed manual cleaning before any broad application method
Fogging or misting is not a shortcut for physically removing soil and residue.Treatment of overlooked surfaces and hidden contact areas
Bed frames, drawer pulls, caster wheels, mattress seams, lift points, and fabric interfaces often need hands-on attention.Verification steps
Facilities that use ATP testing or other validation methods gain a better record that the room wasn't just cleaned. It was evaluated.
For a broader look at why superbug cleanup requires more than ordinary cleaning, this guide to cleaning infectious bacteria and superbugs is worth reviewing.
When professional intervention is non-negotiable
Certain scenarios shouldn't be handed to routine housekeeping or untrained staff:
- A room is being turned over after known MRSA occupancy and there are concerns about thoroughness.
- The setting includes high-risk residents, immunocompromised occupants, or behavioral health populations with heavy surface contact.
- There has been wound drainage, blood, bodily fluid release, or extensive contamination of porous contents.
- The site involves a residence, multifamily unit, or mixed-use property where contamination boundaries are unclear.
- Leadership needs documentation that supports compliance, insurance, and defensible reoccupancy decisions.
That isn't alarmism. It's risk management. The cost of under-responding often appears later, when another occupant becomes ill, a regulator asks for documentation, or a property transfer raises questions no one can answer cleanly.
Protocols for Biohazardous Waste and Laundry
What leaves an MRSA room can spread the problem if the exit path isn't controlled. Waste and laundry protocols are where many otherwise careful facilities get casual. They bag too late, carry items uncovered, overfill containers, or let contaminated linens brush uniforms and hallway surfaces.
Waste handling inside the room
Bag waste at the point of use whenever possible. Staff shouldn't carry loose contaminated items into corridors to sort them later. If material is wet, leaking, or visibly contaminated, containment needs to prevent seepage during transport and staging.
Core practices include:
- Bag in the room so the contamination boundary stays intact.
- Use appropriate labeled containers or bags according to facility policy and applicable regulations.
- Don't compress waste by hand because that creates puncture and splash risk.
- Close and transfer carefully so the exterior stays clean enough to handle safely.
If sharps are involved, use approved sharps containers. If blood or other potentially infectious material is present, the handling standard becomes even stricter. Staff need to know that "MRSA waste" isn't a casual label. The actual disposal category depends on what the waste contains and how the jurisdiction regulates it.
For a practical overview of compliant handling and final disposition, biohazard waste disposal requirements are worth reviewing.
Laundry needs a separate workflow
Linens are one of the easiest ways to move contamination out of isolation if they're shaken, hugged against clothing, or dropped onto the floor. The rule is simple. Handle as little as possible, and contain as early as possible.
A workable laundry process looks like this:
- Wear the required PPE while handling used linens.
- Avoid shaking or sorting in the room.
- Place linens directly into designated bags or hampers suitable for contaminated laundry.
- Close the bag before transport and keep the outside of the bag clean.
- Send to a laundry operation that follows healthcare-grade procedures for contaminated textiles.
Linens don't need dramatic handling. They need quiet, controlled handling.
Documentation matters
Facilities should be able to show who handled waste, where it was staged, who transported it, and what vendor or internal process completed final disposal or laundering. In a review after an exposure concern, written records carry more weight than verbal reassurance.
Property managers and residential families often don't realize this until after the fact. If a death, unattended illness, or severe contamination event occurred in a home or unit with suspected MRSA involvement, ordinary trash and laundry decisions can create unnecessary secondary exposure. That's one of the clearest points where professional guidance protects everyone involved.
Sustaining Safety Through Training and Monitoring
A written protocol can be perfect and still fail on a busy shift. Staff swap assignments, float between units, improvise supply storage, and learn habits from each other. That's why MRSA control isn't a one-time rollout. It's an ongoing training and monitoring program.
What staff training has to cover
Training should be practical, room-based, and repeatable. If employees only see the protocol in a binder or annual slideshow, the facility is depending on memory under stress.
A useful training program covers:
- How to identify when MRSA isolation precautions apply
- Correct donning and doffing
- Hand hygiene at the actual room threshold
- Dedicated equipment rules
- Cleaning boundaries for nursing, EVS, and outside vendors
- Waste and laundry routing
- Visitor coaching
- Escalation procedures when a room requires terminal decontamination
Managers should include nonclinical workers too. Maintenance staff, transport aides, security, agency workers, and contractors often cross the threshold where contamination control matters.
For organizations building stronger competency systems, training in biohazard cleanup and compliance offers a useful framework.
Monitoring what people actually do
Audits should focus on real behavior, not paper completion. Watch the doorway. Watch the glove change. Watch whether hand hygiene happens after touching the curtain or exit handle. Watch how EVS handles reusable tools and whether dirty and clean supplies stay separated.
Monitoring can include:
- Direct observation rounds
- Supply checks at room entry
- Spot reviews of signage clarity
- Environmental cleaning checklists
- Competency refreshers after observed errors
The best audit question is simple. Could a new employee walk up to this room and do the right thing without guessing?
That question reveals whether the system is carrying the worker, or the worker is carrying the system.
The harder question of when precautions can stop
Facilities need judgment, not reflexes. Isolation shouldn't continue forever just because someone once tested positive. At the same time, stopping precautions too casually can expose high-risk occupants.
Recent SHEA updates acknowledge a more risk-based approach. In some low-transmission hospital units, teams have dropped gowns and gloves for MRSA-colonized patients without seeing an infection rate spike, with 0.8% versus 1.2% baseline in multi-facility trials (discussion of removing unnecessary contact isolation). The practical takeaway isn't that precautions no longer matter. It's that some organizations are moving toward evidence-based de-isolation rather than indefinite automatic restrictions.
How to make de-isolation decisions safely
A sound de-isolation review should consider:
- Current symptoms and wound status
- Whether drainage can be fully contained
- The vulnerability of nearby occupants
- The type of unit or setting
- Whether the person still requires frequent high-contact care
- Facility policy and medical oversight
- Whether environmental remediation has been completed when indicated
In nonclinical settings, this often means the answer isn't "just reopen the room." It means assess the risk, clear the environment properly, document what was done, and only then return the space to normal use.
Frequently Asked Questions About MRSA Protocols
FAQ Quick Reference
| Question | Key Takeaway |
|---|---|
| Does every MRSA-positive person need strict isolation? | No. The setting, symptoms, drainage, and contact risk all matter. |
| Can routine housekeeping handle post-discharge cleanup? | Not always. Terminal decontamination is a separate task when risk or contamination is significant. |
| Are gowns and gloves enough by themselves? | No. PPE only works with proper use, hand hygiene, and environmental controls. |
| Should offices or homes react the same way hospitals do? | No. The response should match the exposure risk and the type of contact happening in the space. |
| When should a professional remediation team be called? | When contamination is extensive, porous materials are involved, vulnerable people remain on site, or documentation and compliant clearance are needed. |
Does an MRSA-positive person always need a private room?
Not always, but many settings prefer one when available because it reduces contact variables. The decision depends on the person's condition, whether wounds or drainage can be contained, the amount of direct care required, and who else occupies the space. In a nonclinical residence, "private room" usually means limiting access and controlling what enters and leaves that area.
Is MRSA only a hospital problem?
No. It shows up in long-term care, behavioral health settings, outpatient environments, multifamily housing, and private homes. The management approach changes by setting, but the core concerns remain the same: contact spread, contaminated surfaces, shared items, and whether the environment has been cleaned at the right level.
Can a janitorial crew do the final cleanup after discharge?
Sometimes for low-risk routine turnover, but not for every case. If there was active drainage, broad surface contamination, compromised porous contents, bodily fluids, uncertainty about spread, or high-risk future occupants, standard janitorial turnover may not be enough. That's where certified biohazard remediation becomes the safer option.
If the question is whether cleaning was "probably enough," the documentation and clearance process probably wasn't strong enough.
What should families do in a home setting?
Keep the response simple and controlled. Limit unnecessary contact with the affected area, avoid sharing personal items, contain used linens carefully, and follow medical guidance for wound care and hygiene. If the home has visible contamination, a deceased occupant, heavy clutter, hoarding conditions, or any situation where normal cleaning can't confidently restore safety, bring in professionals.
Can soft furniture and personal belongings stay in the room?
Some items can remain after proper assessment and treatment. Others shouldn't. Porous materials are harder to decontaminate than hard, nonporous surfaces, especially if they were directly contaminated. Mattresses, upholstered chairs, cushions, stuffed items, and layered fabric contents deserve careful review, not assumptions.
When is professional intervention the right call?
Call trained remediation professionals when:
- The contamination extends beyond ordinary touchpoints
- Blood, bodily fluids, drainage, or medical waste are involved
- The property includes vulnerable occupants
- The room is being returned to service and liability matters
- You need documentation for insurers, regulators, or property records
- Staff or family members aren't equipped to assess salvage versus disposal
Can precautions be lifted just because the room looks clean?
No. Visual appearance isn't a clearance standard. A room can look orderly and still contain contamination on high-touch surfaces, fabrics, equipment seams, and overlooked transfer points. Safe reoccupancy depends on the type of event, how the room was cleaned, and whether the response matched the risk.
When MRSA contamination goes beyond daily staff-managed precautions and into terminal cleaning, waste handling, or post-incident decontamination, 360 Hazardous Cleanup provides the kind of compliant, discreet, trauma-informed response that protects people, property, and documentation. Their team works with healthcare facilities, property managers, insurers, and families who need more than a surface wipe-down. They need a space that has been assessed carefully, remediated correctly, and cleared with safety at the center of every decision.
