In long term care, infection risk isn't an occasional disruption. It's part of daily operations. The CDC estimates that 1 in 43 nursing home residents has at least one infection on any given day, and across U.S. healthcare settings, about 1 in 31 patients has at least one healthcare-associated infection on any given day, according to the CDC's healthcare-associated infection progress data.
That changes how facility leaders should think about the job. Infection prevention isn't a binder on a shelf, and environmental cleaning isn't just housekeeping. In a nursing home, assisted living setting, or behavioral health residence with hands-on care needs, long term care infection control has to function as a living system. It has to cover routine prevention, surveillance, escalation, outbreak response, and the point where in-house staff should stop and bring in certified biohazard remediation support.
The Reality of Infection Risk in Long Term Care
The first mistake I see is treating infection control as a narrow clinical function. It isn't. It's an operational discipline that reaches nursing, environmental services, rehab, dietary, maintenance, admissions, wound care, transportation, and leadership.
Residents move. Staff float. Families visit. Devices need attention. Wounds need dressing changes. Linens and briefs need frequent handling. Shared bathrooms, therapy spaces, carts, lifts, touchpoints, and transport routes all create transmission opportunities. That means your program has to work in the actual building, with the actual staff you have, on the hardest day of the month, not just during a planned audit.
A second mistake is waiting for a confirmed outbreak before tightening the system. By then, you've already lost time.
Practical rule: If your team is only reacting to lab confirmations, new orders, or obvious symptoms, your surveillance is late.
Continuous observation matters because infection signals in long term care are often subtle at first. A resident's appetite changes. A wound looks worse. Two staff members call out ill on the same hall. A room turnover reveals heavier contamination than expected. Those are operational clues, not side notes.
For wound-related concerns, frontline staff and families often need a plain-language reference that helps them recognize early warning signs without guessing. EkagraHealth AI's wound care information is a useful example of practical education that can support escalation decisions alongside clinical judgment.
Facility leaders also need to recognize when contamination crosses from infection prevention into biohazard response. Blood, body fluids, feces, emesis, trauma scenes, and heavily contaminated resident spaces may require controls beyond normal environmental services. The risks tied to these events overlap with many of the diseases commonly associated with biohazard scenes, which is why escalation criteria should be written before a crisis starts.
Developing Your Facility's IPC Framework
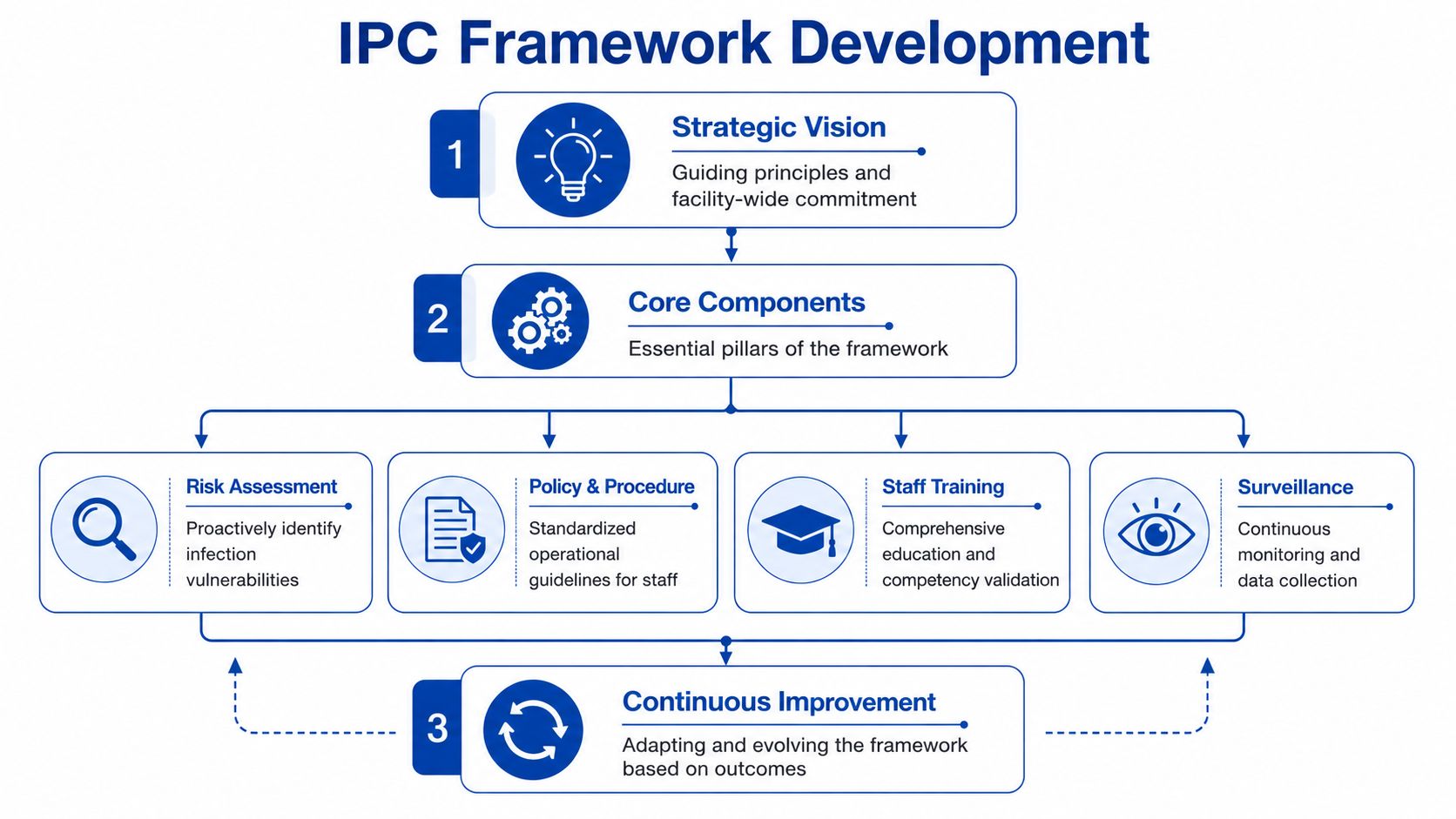
A workable infection prevention and control program starts with a risk assessment, not a template. Generic policies fail because they don't match the building, the resident population, or the staffing reality.
Start with your actual vulnerabilities
Look at who you care for and how care is delivered. A facility with a high number of residents who need wound care, toileting assistance, feeding support, or device management has a different risk profile than a lower-acuity setting. The same is true for memory care units, shared bathing areas, and frequent off-site appointments.
Your assessment should answer questions like these:
- Resident factors: Who has wounds, devices, incontinence, cognitive impairment, frequent antibiotic exposure, or repeated transfers?
- Building factors: Where are the choke points, shared equipment routes, therapy spaces, clean-to-dirty workflow breaks, and storage limitations?
- Operational factors: Which shifts struggle most with compliance, handoff communication, supply access, and room turnover?
A good framework also defines what happens when normal work conditions degrade. PPE shortages, staff call-offs, delayed laundry, agency staffing, and unit closures all affect infection risk.
Build policies people can actually use
Policies have to be specific enough for surveys, but simple enough for shift use. If staff can't find the correct procedure in under a minute, the document isn't doing its job.
At minimum, written policies should cover:
| Program element | What the policy should define |
|---|---|
| Surveillance | What infections are tracked, who reviews trends, how clusters are escalated |
| Precautions | Standard precautions, transmission-based precautions, and resident-specific barrier practices |
| Environmental cleaning | Routine cleaning, enhanced disinfection triggers, product use, dwell times, documentation |
| Exposure response | Blood and body fluid cleanup, staff exposure reporting, immediate containment |
| Outbreak actions | Chain of command, public health notification, cohorting, communication workflows |
One practical way to strengthen defensibility is aligning facility procedures with broader workplace exposure expectations. Leaders reviewing cleanup, PPE, and incident response protocols should understand how these responsibilities connect with OSHA guidelines for biohazard exposure and workplace incidents.
Policies fail when they describe an ideal process that your night shift can't perform.
Treat the plan as a live operating document
The strongest programs don't separate policy from training, audits, and corrections. If hand hygiene audits reveal misses during wound care, update the teaching. If EVS staff can't access the right disinfectant at the point of use, fix the storage workflow. If a room restriction policy keeps getting bypassed because residents wander, revise the approach rather than pretending compliance exists.
The framework should tell every department three things clearly. What to watch for. What to do now. Who to call next.
Implementing Daily Prevention and Barrier Protocols
Daily prevention succeeds when staff can connect the rule to the task in front of them. "Wash your hands" is too generic. "Clean hands before wound care, after glove removal, after contact with the resident environment, and before touching supplies on the cart" is actionable.
A strong review of long-term care infection prevention found 74 studies, including 34 non-outbreak studies and 40 outbreak studies, and reported that hand hygiene was the most commonly studied non-outbreak intervention at 10 studies, with all but one reporting reduced infection rates. The same review also found benefit in oral hygiene in 6 studies and successful resident vaccination in 3 studies, supporting layered prevention rather than a single tactic, as detailed in the systematic review on infection prevention and control in long-term care facilities.

Hand hygiene has to be tied to care moments
Most facilities already have dispensers, posters, and annual competencies. That's not the same as a functioning hand hygiene program. The gap is usually between policy and task flow.
Managers should audit hand hygiene during real work, not staged observations. Watch med pass. Watch dressing changes. Watch feeding assistance. Watch glucometer handling. Watch how often staff clean hands after touching bed rails, wheelchairs, lift slings, and privacy curtains.
Focus your coaching on friction points:
- Glove misuse: Gloves don't replace hand hygiene. Staff often contaminate carts, door handles, and mobile devices while gloved.
- Supply placement: If sanitizer and PPE aren't at the point of care, compliance drops under time pressure.
- Interrupted tasks: Long care sequences create contamination creep. Staff need clear break points for glove changes and hand cleaning.
Use barrier precautions that fit real nursing home care
Traditional isolation language can sound clean on paper and fail in practice. Many residents need frequent assistance and can't tolerate prolonged room restriction. That's why managers need practical barrier protocols for high-contact care, not just a default order to isolate.
Enhanced precautions should be built around tasks such as dressing changes, bathing, toileting, linen changes, and device access. During these encounters, staff need the right PPE, the right sequencing, and a clear process for handling contaminated linens and surfaces before moving to the next resident.
A common weak spot is blood or body fluid cleanup during busy care periods. Staff should know the difference between immediate containment and full decontamination, and they should have a simple reference for the procedure for cleaning blood spills so they don't improvise under pressure.
Residents don't get safer because a door sign went up. They get safer when the staff member providing hands-on care uses the right barrier at the right moment.
This training video can help reinforce hand hygiene technique and observation basics for frontline education sessions.
Daily prevention is a bundle, not a hero move
The facilities that perform best don't rely on one vigilant nurse or one strict manager. They make infection control routine by turning it into small, repeatable actions.
That usually includes:
- Consistent oral care: Especially where aspiration risk and dependency are common.
- Resident vaccination workflows: Not just recommendations, but tracking, follow-up, and family communication.
- Equipment discipline: Cleaning shared blood pressure cuffs, lifts, commodes, and therapy devices between uses.
- Shift-level accountability: Charge nurses and supervisors need authority to correct unsafe practice in real time.
If your staff can explain why each barrier exists during a specific care task, your program is maturing. If they can only recite the policy title, it isn't.
Environmental Control From Routine Cleaning to Hazmat Response
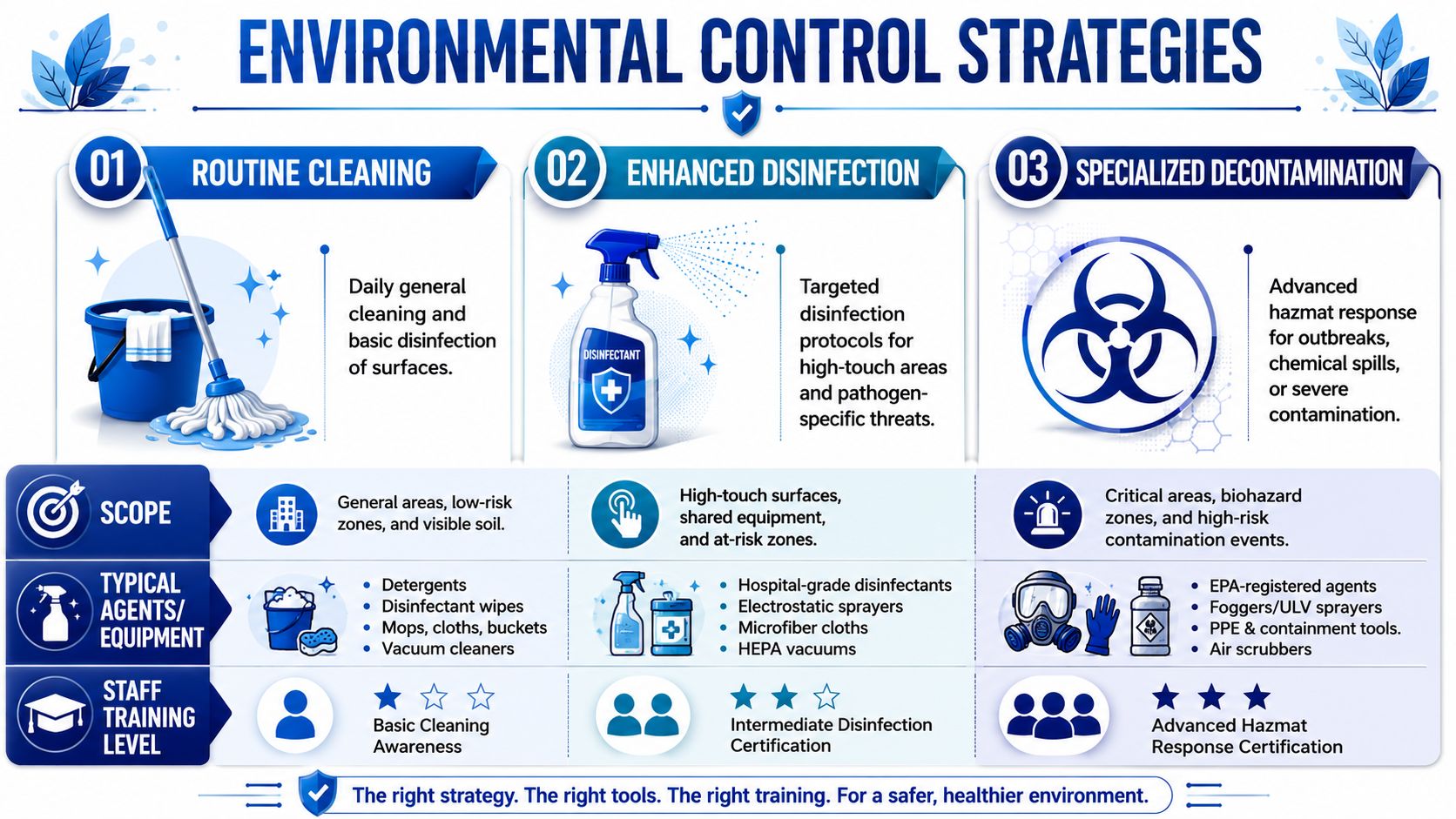
Environmental cleaning in long term care has three levels. Routine cleaning, enhanced disinfection, and specialized decontamination. Problems start when facilities treat all three as the same job.
What in-house teams should own every day
Routine environmental control belongs inside the facility. That includes scheduled cleaning of resident rooms, shared bathrooms, dining areas, nursing stations, rehab spaces, and high-touch surfaces. It also includes auditing whether products are mixed and used correctly, whether contact times are followed, and whether cleaning tools move safely from dirty to clean areas.
Enhanced disinfection starts when risk rises. A symptomatic resident, repeated contamination of a bathroom, heavy fecal soiling, emesis events, or a cluster on one hall may require more frequent disinfection, tighter documentation, dedicated equipment, and room-specific workflows.
That level of response is still manageable in-house if three conditions are true:
| Level | Typical scope | Who should handle it |
|---|---|---|
| Routine cleaning | Daily housekeeping and standard disinfection | Facility EVS and trained nursing support |
| Enhanced disinfection | Targeted response to active contamination or elevated transmission concern | Facility team with infection prevention oversight |
| Specialized decontamination | Large-scale biohazard contamination, trauma scenes, severe outbreak contamination, unsafe waste handling conditions | Certified biohazard remediation professionals |
Where facilities get into trouble
The most common error isn't lack of effort. It's asking overstretched staff to perform a decontamination job with janitorial staffing, janitorial time, and janitorial equipment.
A 2024 analysis discussed in Infection Control Today's review of infection prevention in outpatient and long-term care settings found that 26.5% of skilled nursing or nursing homes reported never experiencing certified nursing assistant shortages and 18.8% reported never experiencing registered-nurse shortages, which means many facilities face staffing disruption that can weaken surveillance, cleaning consistency, and outbreak response.
When staffing becomes fragile, the environmental program is usually one of the first systems to drift. Terminal cleaning gets delayed. Shared equipment misses disinfection. Isolation carts aren't restocked. Waste handling shortcuts appear. Documentation gets completed after the fact.
If contamination is spreading faster than your team can contain and verify, you no longer have a routine cleaning problem.
Support services outside resident care matter too. Dietary areas, waste staging zones, and loading corridors can become overlooked links in the contamination chain. Facilities reviewing sanitation standards in food service spaces may also benefit from operational resources such as Crown Point commercial kitchen pest control, because infection prevention breaks down quickly when environmental hygiene is fragmented across departments.
When to escalate to professional biohazard remediation
There should be no ambiguity here. Call specialized remediation support when the contamination exceeds your staff's training, equipment, legal handling capacity, or ability to maintain safe operations while cleaning.
Escalation is appropriate when you have situations such as:
- Multi-room or multi-wing contamination: Repeated vomiting or fecal contamination events that outpace turnover and disinfection capacity.
- Persistent high-burden contamination: Rooms, bathrooms, or common areas with extensive organic material, porous-surface involvement, or recurrent recontamination.
- Trauma or medical accident scenes: Events involving significant blood or body fluids that require regulated waste handling and deep decontamination.
- Organism-specific concerns: Circumstances where environmental persistence and transmission risk require a more controlled response, including scenarios that may warrant focused C. difficile cleaning.
- Operational collapse risk: When taking staff off the floor to clean would jeopardize resident care, medication delivery, or surveillance.
In those moments, professional remediation isn't a luxury add-on. It's part of risk control. A provider such as 360 Hazardous Cleanup can perform regulated biohazard cleanup, waste handling, containment support, and infectious-disease decontamination when the event surpasses what internal teams should safely manage.
The key distinction is simple. Routine EVS work maintains a safe environment. Certified biohazard remediation restores control after a serious contamination event.
Managing Active Outbreaks and Antimicrobial Resistance
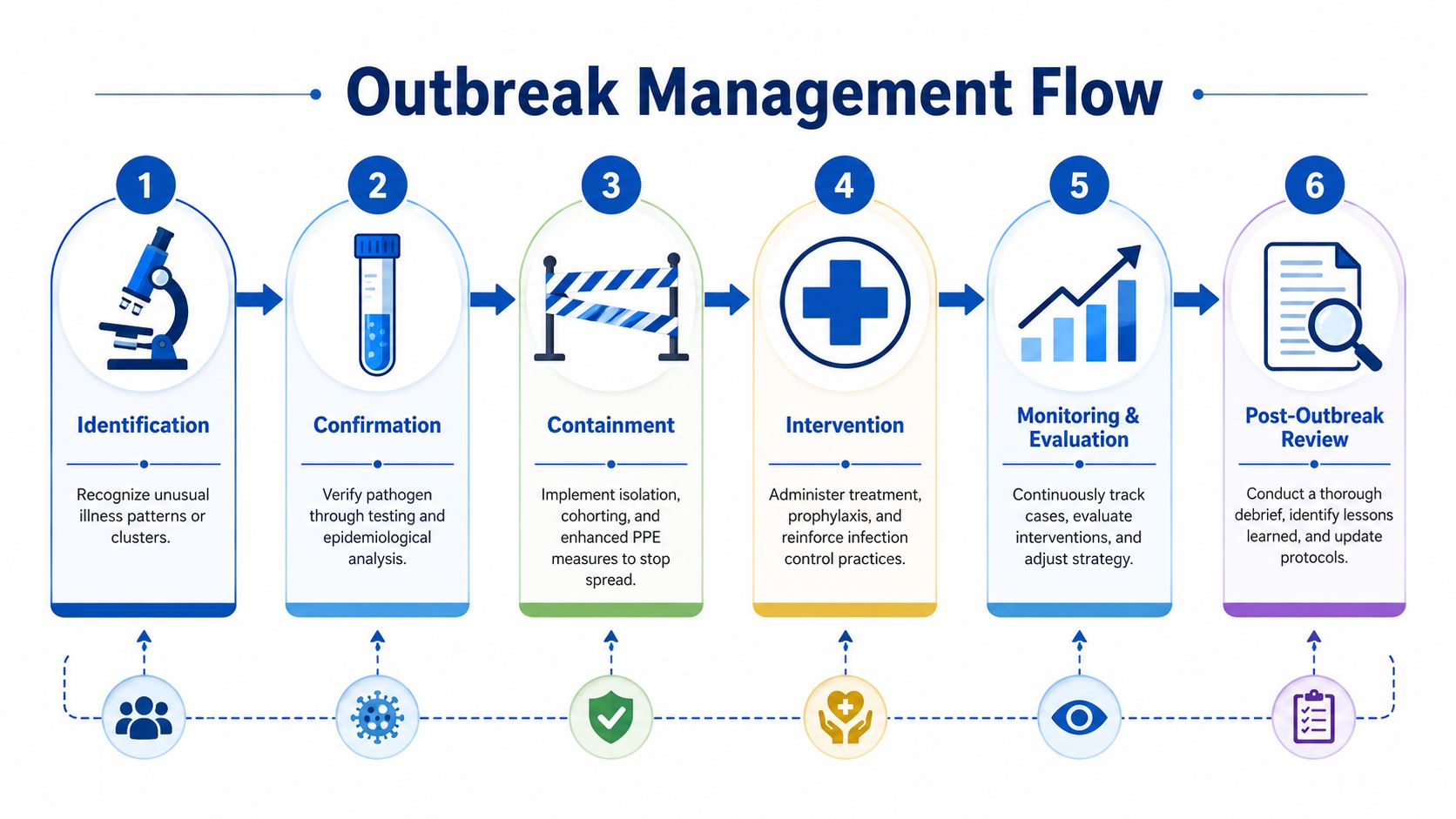
When a possible outbreak starts, speed matters more than polish. The first hours should focus on detection, containment, and clean communication.
Build your response around a working case definition
Start with what staff can identify consistently. That may be a cluster of similar symptoms on one hall, a sudden increase in new antibiotics, repeated loose stools, unusual respiratory illness patterns, or multiple staff illnesses linked to the same unit.
Then lock down the basics:
- Identify cases consistently. Define who is included and from what date.
- Separate risk where possible. Cohort residents, dedicate equipment, and control movement.
- Tighten PPE and cleaning workflows. High-touch and shared-use items need immediate attention.
- Notify the right parties. Leadership, medical staff, pharmacy, frontline supervisors, and public health contacts should hear the same message.
A sloppy case definition creates sloppy control measures. Staff end up applying different rules on different shifts, and confidence drops.
Stewardship belongs inside outbreak control
Cleaning matters. Testing matters. PPE matters. None of that replaces antibiotic stewardship.
AHRQ guidance for long-term care emphasizes that infection prevention programs should integrate antibiotic stewardship because inappropriate antibiotic use drives resistance, and facilities are advised to maintain written surveillance plans and reassess infection priorities annually, as described in AHRQ's long-term care infection prevention guidance.
That has practical implications during an outbreak:
- Review new antibiotic starts: Ask why each was started, what syndrome is being treated, and whether the evidence supports it.
- Track resistant organisms: If your facility is seeing repeated resistant infections or colonization concerns, your surveillance plan should reflect that.
- Avoid reflexive over-treatment: Not every fever, cough, or urine change justifies broad antibiotic use.
- Balance precautions with quality of life: Use transmission-based measures when indicated, but don't let fear drive unnecessary restrictions without a plan.
Facilities also benefit from keeping staff education grounded in real transmission pathways, especially when resistant organisms are involved. A practical reference on cleaning superbugs and infectious bacteria can help managers reinforce why cleaning choices and stewardship decisions have to work together.
Outbreak management fails when the facility treats antibiotics as a substitute for surveillance.
Communicate like an operator, not a marketer
Residents, families, and staff don't need vague reassurance. They need timely, accurate instructions.
Tell staff what symptoms to report, what PPE is required, what spaces are restricted, and who is monitoring new cases. Tell families what has changed in visitation or resident movement and why. Tell your governing body what resources are under strain. The calmer your communication system is, the less likely people are to invent their own workflow.
After control measures are in place, keep reviewing line lists, exposures, staffing impact, and environmental burden. If the event grows beyond internal capacity, that decision should trigger operational support, not debate.
Sustaining Compliance and Ensuring Program Readiness
Strong long term care infection control programs don't rely on memory. They rely on repeated verification. If you want a program to survive turnover, survey pressure, and outbreak stress, it has to be embedded in routine management.
That means infection prevention belongs inside your quality process. Audit findings should go to leadership. Repeat failures should trigger corrective action. Supply gaps, missed cleaning steps, weak hand hygiene moments, poor documentation, and delayed escalation should all feed into a structured review cycle.
Audit what staff actually do
Annual policy review isn't enough. Readiness lives in the gap between written process and observed behavior.
Use short, repeatable audits on live work such as:
- Barrier use during hands-on care: Watch dressing changes, toileting, bathing, and device access.
- Environmental cleaning verification: Confirm product choice, sequence, and completion in high-risk rooms.
- Shift communication: Check whether new infections, new antibiotics, and new precautions are handed off reliably.
- Supply control: Make sure PPE, disinfectants, waste containers, and linen handling supplies are where the work happens.
Guidance in this area increasingly emphasizes that prevention must work during high-contact care for residents who can't realistically be isolated, and the CDC-linked Enhanced Barrier Precautions model focuses on safer routine care for residents with wounds, indwelling devices, or MDRO concerns, as explained in the multisociety discussion of Enhanced Barrier Precautions in nursing homes.
That point matters for compliance. Survey readiness isn't just about showing you know isolation rules. It's about showing you can prevent transmission during ordinary resident care.
Readiness includes external response capacity
Every facility should know, before an incident occurs, where in-house responsibility ends. If you wait until a traumatic event, severe contamination, or large-scale infectious cleanup need arises, you'll lose critical time sorting out approvals, access, waste handling, and documentation.
A practical readiness checklist looks like this:
- Written escalation triggers: Define the events that require outside decontamination support.
- Approved vendors and contacts: Keep response partners current and accessible after hours.
- Leadership authority: Clarify who can authorize emergency remediation.
- Documentation workflow: Make sure incident reports, chain of communication, and waste records can be completed correctly.
The facilities that stay steady under pressure don't separate prevention from response. They connect them. Daily audits inform better policy. Better policy improves frontline execution. Stronger execution catches problems sooner. Clear escalation criteria prevent a difficult event from becoming a prolonged failure.
When that cycle works, compliance improves, resident safety improves, and the building remains operational under strain.
When a contamination event exceeds normal housekeeping or nursing capacity, a facility needs a partner that can step in quickly, work within regulatory requirements, and protect residents, staff, and operations. 360 Hazardous Cleanup provides professional biohazard remediation and infectious-disease cleanup support for situations that require more than routine environmental services, including large-scale contamination, exposed bodily fluids, and crisis-driven decontamination needs in healthcare and long-term care settings.
