A tenant calls before sunrise. There's been a medical emergency in one unit, blood on the bathroom floor, and family members are on the way. Your maintenance lead wants to help. Your front office wants the hallway reopened fast. Your first instinct may be to grab gloves, disinfectant, and a mop.
That instinct is understandable. It can also create a second incident.
In moments like this, infection control compliance stops being a clinical phrase and becomes a management responsibility. You're not just deciding how to clean a surface. You're deciding who may be exposed, what must be documented, what waste is regulated, and whether your actions protect people or increase risk.
The stakes are real. In U.S. acute care hospitals, approximately 1 in 31 patients has at least one healthcare-associated infection on any given day, leading to about 72,000 deaths annually, according to CDC data on healthcare-associated infections. Your property isn't a hospital, but those figures show what happens when pathogen control breaks down.
Property managers often tell me the hardest part isn't the willingness to act. It's knowing where routine janitorial work ends and regulated response begins. That line matters after trauma scenes, unattended deaths, bodily fluid incidents, hoarding cases, and infectious contamination concerns. It also matters for staff safety, tenant confidence, insurance documentation, and legal exposure.
If your team already thinks about occupant health, ventilation, and surface hygiene, you're not starting from zero. Resources on how commercial cleaning combats COVID-19 can help frame how contamination moves through shared spaces. But post-incident scenes demand a more disciplined standard than everyday cleaning.
Practical rule: If an incident involves blood, bodily fluids, unknown biological material, or a death scene, treat it first as a safety and compliance issue, not a housekeeping task.
Beyond the Cleaning Closet An Introduction to Compliance
A warehouse supervisor finds blood droplets near a loading bay after an injury. An apartment manager enters a unit after neighbors report odor and discovers decomposition-related contamination. A behavioral health facility has a self-harm event in a restroom. These situations don't look alike, but they create the same immediate pressure. Secure the area, protect people, and make decisions quickly.
Why the first response matters
The first mistake I see is assigning a trauma-related cleanup to the closest available employee. That person may be hardworking and loyal. They still may not know how to assess porous materials, isolate a pathway, prevent cross-contamination, or package regulated waste correctly.
The second mistake is focusing only on what's visible. Biohazards rarely stay where the eye stops. Fluids can wick under baseboards, enter grout lines, soak padding, contaminate tools, or spread on shoes and cart wheels into common areas.
A compliant response starts with a few basic actions:
- Restrict access: Keep tenants, visitors, and untrained staff out of the area.
- Pause routine cleaning: Standard supplies and open carts can spread contamination.
- Identify who has authority: One decision-maker should coordinate safety, documentation, and vendor communication.
- Preserve records: Photos, incident notes, and service logs may matter for insurance and internal review.
Compliance is risk management with a human face
People sometimes hear “compliance” and think fines or paperwork. Those matter, but they're not the main point. The primary purpose is to prevent avoidable exposure and reduce the chance that one event becomes many.
For property managers, that means asking different questions. Was the scene isolated properly? Did anyone enter without protection? Were exposed materials removed lawfully? Can you show that the response was handled in a defensible way if an insurer, regulator, or family member asks later?
A clean-looking room can still be an unsafe room if the response ignored exposure pathways, waste handling, or staff protection.
What Infection Control Compliance Really Means
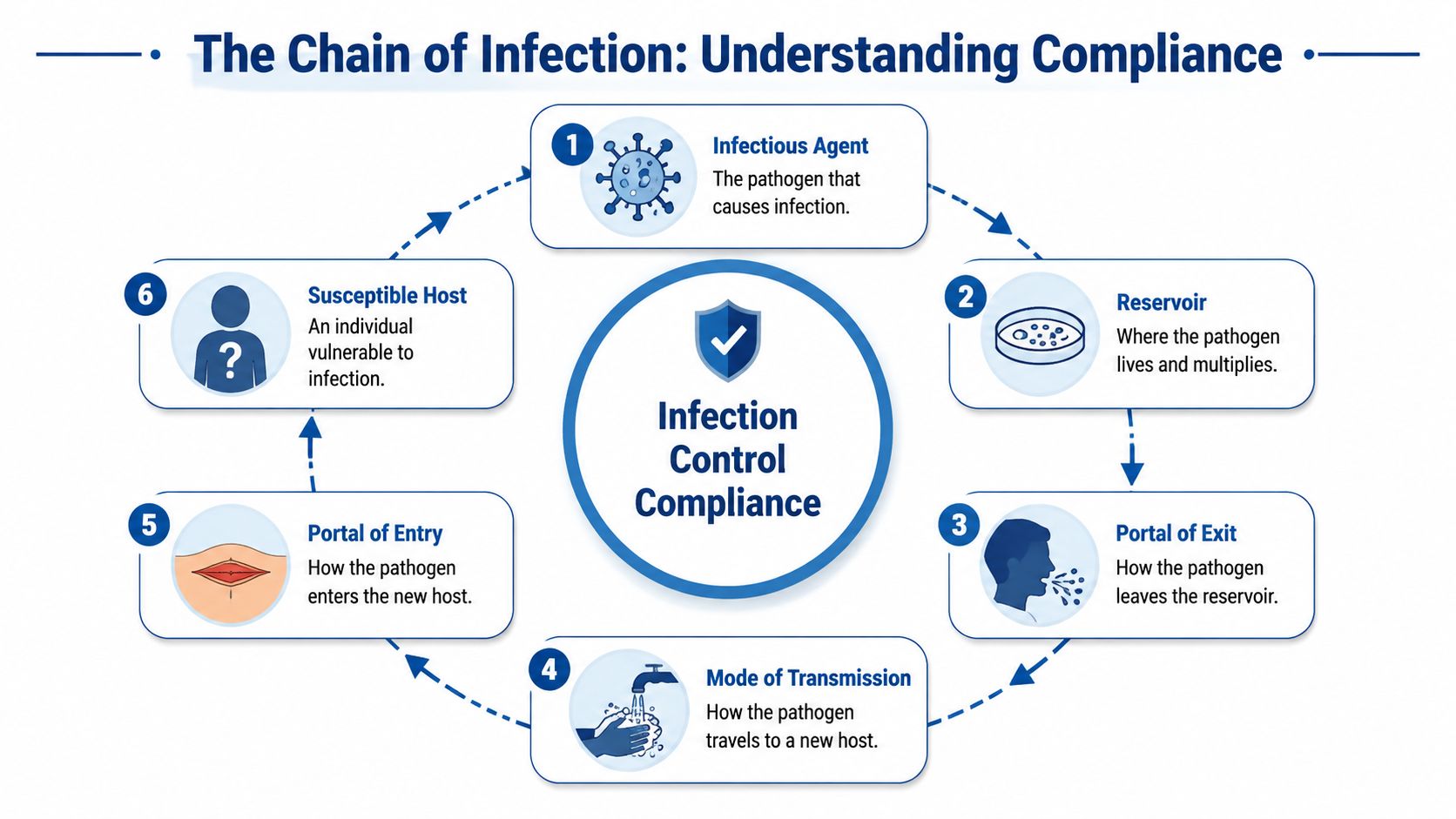
Infection control compliance makes more sense when you stop thinking about products and start thinking about pathways. Infection spreads through a chain. Compliance exists to break that chain before it reaches another person.
The chain of infection in plain language
A simple way to think about a contaminated scene is the chain of infection:
| Link | What it means on a property |
|---|---|
| Infectious agent | The bacteria, virus, or other pathogen |
| Reservoir | The place it survives, such as blood, tissue, waste, or a contaminated surface |
| Portal of exit | How it leaves that source |
| Mode of transmission | How it travels, such as touch, droplets, tools, shoes, or carts |
| Portal of entry | How it gets into another person |
| Susceptible host | The person who becomes exposed |
Every sound protocol tries to break one or more of those links. Gloves interrupt contact. Containment limits spread. Disinfection targets the pathogen itself. Proper waste packaging removes contaminated material from the environment. Hand hygiene protects the next surface, the next room, and the next person.
That's why a trauma scene can't be reduced to “wipe it down.” A visible stain is only one part of the chain.
Cleaning, sanitizing, and disinfecting are not the same
These terms get mixed together constantly, and that confusion causes bad decisions.
- Cleaning removes dirt, residue, and some contaminants from a surface.
- Sanitizing lowers microbial presence to a level considered safer for routine settings.
- Disinfecting uses an appropriate product and contact process to kill or inactivate targeted pathogens on a prepared surface.
In a break room, routine cleaning and sanitizing may be enough for many surfaces. In a blood or bodily fluid incident, the standard changes. Soil has to be removed first, then the correct disinfection process has to be carried out according to the product label and the condition of the material.
Porous items complicate things further. Upholstery, subflooring, ceiling tile, insulation, and unfinished wood may not be salvageable after contamination. That decision shouldn't be based on appearance alone.
For a deeper look at field procedures, biohazard cleanup best practices and guidelines for safe and effective cleanup offers a practical reference point for managers who need to understand what trained crews do on site.
What readers often get wrong
The most common misunderstanding is assuming stronger chemicals automatically mean better compliance. They don't. The wrong product, poor dwell time, skipped pre-cleaning, or improper PPE can make an aggressive-looking response noncompliant.
Another confusion point is scope. Infection control compliance isn't limited to the room where the event happened. It includes hallways, shared restrooms, disposal routes, elevator touchpoints, laundry handling, and any staff member who may have entered before the area was secured.
The Regulatory Framework You Must Follow
Most property managers don't need to memorize every regulation. They do need to know which agency governs which part of the problem. That's what keeps a stressful event from turning into a legal and operational mess.
Who governs what
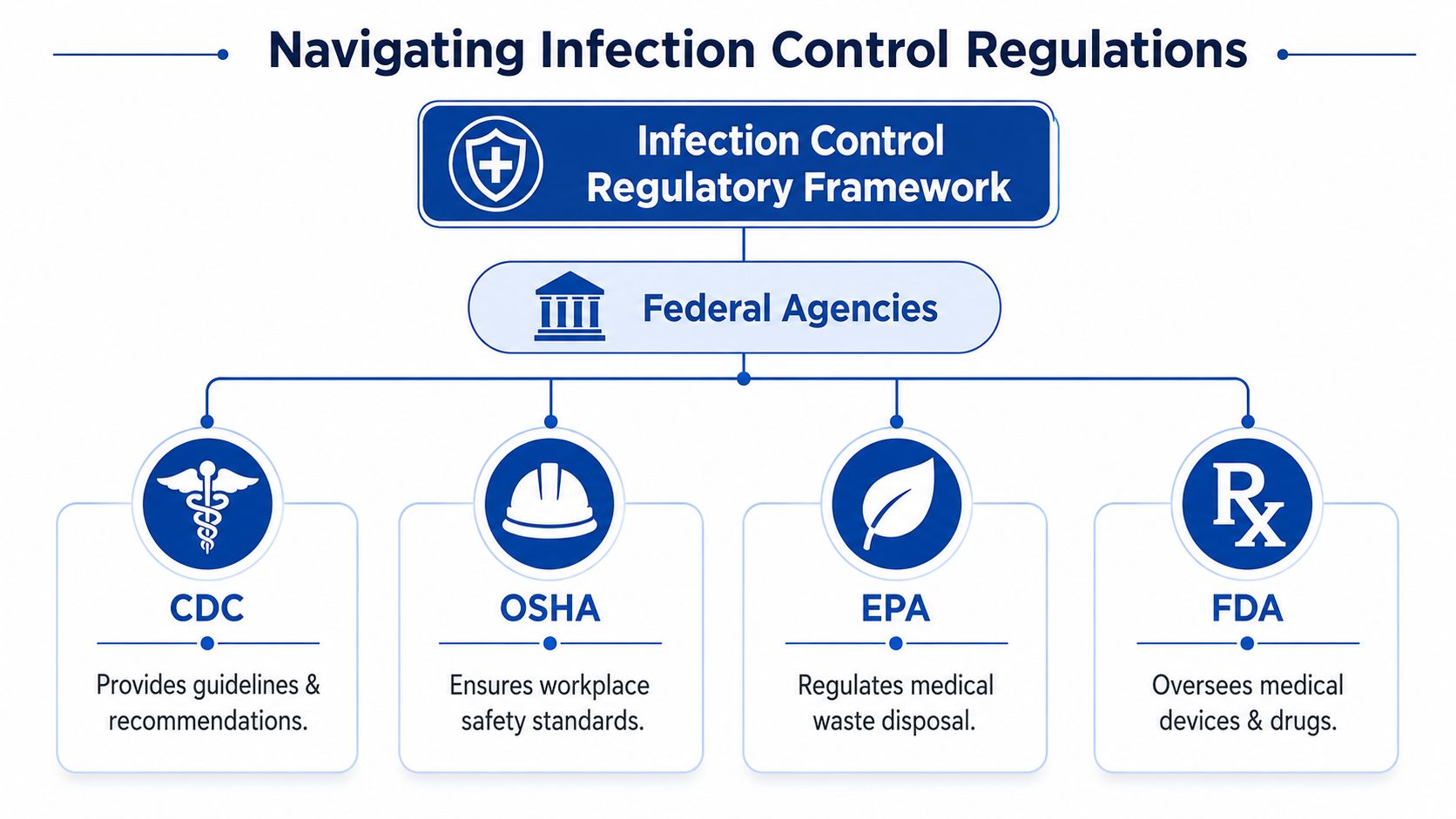
Think of the framework this way:
| Agency or body | What it affects |
|---|---|
| CDC | Infection prevention guidance and core practices |
| OSHA | Worker safety, exposure protection, training, PPE, and workplace procedures |
| EPA | Disinfectant registration and environmental handling requirements |
| FDA | Some medical products and devices used in healthcare settings |
| State and local authorities | Waste transport, reporting, health rules, and added local requirements |
The CDC tells organizations what sound infection prevention looks like. OSHA focuses on whether employers protect workers. The EPA matters because disinfectants and some waste-related practices sit under environmental rules. State and local agencies often add specific disposal, transport, and reporting requirements that can't be ignored.
If you oversee a clinic, long-term care setting, or behavioral health property, the expectations rise. The Joint Commission's revised 2024 infection control standards for healthcare facilities emphasize documented procedures for screening at all entry points, isolation protocols, and PPE use, as outlined in this review of the revised 2024 standards. Even if your site isn't accredited, that standard shows where regulated environments set the bar.
The practical hierarchy for property managers
When I advise a facility team, I usually translate the rules into three responsibilities.
First, protect workers. That means exposure awareness, proper PPE, training, and safe work practices. If an employee might contact blood or other potentially infectious material, this isn't optional.
Second, use approved processes and products. A jug on a janitor's cart isn't enough by itself. The product, the application method, the surface condition, and the waste stream all matter.
Third, match the response to the property type. An office, warehouse, apartment, dialysis clinic, and memory care unit don't have the same traffic pattern, vulnerable population, or documentation burden.
Indoor air also enters the conversation faster than many managers expect. If contamination may have affected circulation, filtration, or aerosolized particles, basic surface response won't answer the whole problem. For a useful overview of commercial indoor air quality standards, it helps to review how air handling intersects with occupant safety.
Operational note: Agencies don't work in isolation. A single incident can trigger worker safety obligations, disinfection requirements, waste rules, and internal reporting duties at the same time.
If you need a property-owner view of worker protection obligations, OSHA and biohazard cleanup compliance and safety standards is a useful place to ground that discussion.
Key Responsibilities in Your Compliance Plan
A workable compliance plan isn't a binder that sits on a shelf. It's a set of decisions your team can execute when people are upset, time is tight, and the scene is changing. Four parts carry most of the load.
Documentation that can stand up later
Documentation is where many otherwise careful teams fall short. If an incident occurs, you need a written process for who secures the area, who authorizes response, how exposure is logged, what vendors are approved, and how waste leaves the site.
That written structure matters because memory gets unreliable under stress. A supervisor may think gloves were available. A porter may remember entering the area before barriers went up. A photo log and incident record settle those questions.
A practical documentation set usually includes:
- Scene records: Time discovered, location, affected materials, and who entered
- Exposure notes: Any employee or contractor with possible contact
- Vendor paperwork: Scope, waste manifest information where required, and service details
- Reentry criteria: Who cleared the area for normal occupancy
Training that changes behavior
Training works when it is specific, repeated, and tied to real tasks. Studies show that healthcare workers who receive adequate Infection Prevention and Control education demonstrate significantly higher adherence to safety protocols, according to this review on IPC compliance determinants.
That principle applies far beyond hospitals. Your leasing staff doesn't need the same depth as a remediation technician, but they do need to know when to stop, isolate, notify, and avoid creating secondary exposure. Maintenance leads need more. Supervisors need still more.
For frontline teams, I like training that covers:
- Recognition of blood, bodily fluids, sharps, decomposition effects, and hidden spread
- Immediate actions such as restricting access and stopping routine cleaning
- Escalation to management, safety, and approved outside responders
- After-action discipline including hand hygiene, incident logging, and not improvising waste disposal
If you want a plain-language refresher on surface transfer and handling mistakes, this guide to cross contamination control methods is a practical companion resource.
PPE and waste are operational tests
PPE is where plans meet reality. If gloves are available but face protection isn't, your plan is incomplete. If supplies exist but staff don't know where they are, your plan is incomplete. If a worker dons equipment but removes it improperly, your plan is still incomplete.
Waste handling is just as revealing. Red-bag concepts, sharps segregation, sealed containers, and lawful transport rules must be understood before an event happens. The moment after a trauma incident is the worst time to ask which bin should be used or whether a contaminated mattress can go into normal trash.
Property owners who want to clarify responsibility lines should review biohazard cleanup and your legal obligations as a property owner.
A Practical Audit Checklist for Your Property
Compliance improves when managers stop relying on general confidence and start asking specific questions. The CDC's Core Infection Prevention and Control Practices recommend that facilities systematically monitor adherence to practices like hand hygiene and appropriate PPE use, using metrics to provide feedback, and the CDC's core practices guidance supports that continuous-improvement approach. An audit checklist is a practical first move.
Walk the site like an inspector would
Don't audit from your desk. Start at the places where an incident would likely be discovered first. Restrooms, stairwells, loading areas, vacant units, wellness rooms, clinics, and housekeeping closets all tell you something different.
Use these questions:
Documentation check
- Is there a written response procedure for blood or bodily fluid incidents?
- Does it name who secures the area and who authorizes outside response?
- Can managers quickly locate incident forms and vendor contact information?
Training check
- Can staff explain the difference between routine cleaning and a biohazard response?
- Do supervisors know who must not handle trauma-related materials?
- Are new hires told how to report a suspected exposure?
Test what happens under pressure
A checklist becomes more useful when you simulate stress. Ask a lead porter where PPE is stored. Ask a weekend supervisor who gets called if a decomposed body is discovered in a unit. Ask the front desk what they'd say to keep bystanders back without disclosing private details.
Then inspect supplies and pathways:
| Area to review | What you're looking for |
|---|---|
| PPE storage | Accessible, stocked, and appropriate to likely incidents |
| Isolation materials | Barrier tape, signage, or methods to secure the area |
| Waste staging | Clear separation from routine trash and public traffic |
| Communication chain | After-hours contacts, vendor list, and internal reporting path |
Don't just ask whether supplies exist. Ask whether a stressed employee could find and use them correctly in the first five minutes.
Look for silent failure points
The most dangerous gaps are often procedural, not visible. An old vendor list. No clear rule about elevator use during waste removal. A maintenance key policy that lets too many people enter a contaminated area before assessment. A habit of “just taking care of it” to avoid alarming residents.
Those habits feel efficient until they aren't. The point of the audit is to make sure your process still works when the person on duty is tired, covering another shift, or facing a scene they've never encountered before.
When Standard Procedures Are Not Enough
Some incidents can be managed with a tightly written internal process and limited cleanup scope. Others cross a line where ordinary procedures stop being safe. That line arrives faster than many teams expect.
Scenes that usually require specialized remediation
The hard cases tend to share one trait. Contamination is deeper, broader, or more uncertain than it first appears.
That often includes:
- Unattended deaths: Decomposition fluids can penetrate flooring, subfloor, wall assemblies, and contents.
- Suicide or trauma scenes: Blood and tissue may travel farther than expected and affect adjacent surfaces.
- Hoarding with biological contamination: Animal waste, human waste, sharps, pests, mold, and blocked egress can coexist.
- Infectious contamination events: Shared bathrooms, resident rooms, or treatment areas may require more than routine disinfection.
Public guidance doesn't always help enough here. Key guidance from bodies like the WHO and CDC focuses on routine clinical infection control but provides limited frameworks for managing post-incident biohazard remediation after events like suicides or unattended deaths, as reflected in The Joint Commission's infection prevention and control focus. That leaves property managers with a gap between general infection control principles and the practicalities of trauma scenes.
Why in-house cleaning reaches its limit
A janitorial team can be excellent at floor care, restroom disinfection, and touchpoint hygiene. That doesn't mean they're prepared for tissue recovery, odor source removal, ATP testing protocols used by some contractors, negative-pressure containment decisions, or regulated packaging and transport.
The hidden issue is porous material. If contamination has entered carpet pad, drywall, insulation, particle board cabinetry, mattresses, or HVAC-adjacent spaces, wiping exposed surfaces won't resolve the hazard. It may only remove the visible reminder.
In such situations, an outside specialist may be necessary. A provider such as 360 Hazardous Cleanup handles trauma scene cleaning, unattended death cleanup, infectious disease cleanup, and regulated waste handling under documented procedures, which is different from routine janitorial scope.
The human factor matters too
A death scene is not just a contamination event. It may also be the site of grief, shock, stigma, or criminal investigation. Sending untrained employees into that environment can cause emotional harm on top of physical risk.
The right question isn't “Can someone clean this?” It's “Can this be remediated safely, legally, and with respect for everyone affected?”
That's the boundary. Once an incident carries biohazard complexity, uncertain spread, structural absorption, or traumatic circumstances, standard procedures are no longer enough.
Choosing a Compliant and Compassionate Partner
When you need outside help, credentials matter. So does conduct. The company you call will work inside a sensitive scene, around residents or staff who may be distressed, and under documentation standards that may follow the job long after the area looks normal again.
What to verify before authorizing work
Start with the basics, but don't stop there.
- Training and safety programs: Ask how technicians are trained for bloodborne hazards, PPE, decontamination, and waste handling.
- Insurance and documentation: Confirm coverage, incident reporting practices, and whether they can support insurer requests.
- Waste chain control: Ask how contaminated materials are packaged, transported, and documented.
- Scope discipline: A credible provider should explain what can be cleaned, what must be removed, and why.
Then ask practical questions that reveal professionalism. Will they protect privacy? Can they coordinate discreet arrival if needed? How do they communicate with family members, residents, or staff on site? Do they understand that your property may still need to function while the scene is being managed?
Signs of a mature remediation partner
The most dependable partners usually communicate in calm, specific terms. They don't dramatize the event. They don't promise shortcuts. They explain what they know, what they need to inspect, and what the next defensible step is.
A strong vetting reference is finding and choosing a trusted cleanup partner and what you need to know. Use it as a buyer's checklist, especially if you've never had to retain a biohazard remediation firm before.
What you're really selecting is not just a cleanup vendor. You're selecting a risk-control partner who will affect occupant safety, staff exposure, documentation quality, and the emotional tone of a difficult day.
When an incident on your property involves blood, bodily fluids, trauma, decomposition, or uncertain contamination, fast action matters. So does getting the response right. 360 Hazardous Cleanup provides 24/7 biohazard remediation with a focus on safety, regulatory compliance, discretion, and trauma-informed care, helping property managers, healthcare facilities, and families move from crisis toward safe reentry.
