You're often handed the problem before you're handed a plan.
A tenant reports blood in a restroom. A maintenance tech finds used sharps behind a loading dock. A supervisor learns that a cleaner wiped up bodily fluids in a vacant unit with standard janitorial supplies because nobody recognized the exposure risk soon enough. In non-clinical environments, that's how bloodborne pathogen risk usually shows up. It's unplanned, emotionally charged, and easy to underestimate.
That's why a bloodborne pathogens exposure control plan matters. Not because OSHA expects a document in a binder, but because your people need clear instructions before they face a situation that can affect their health, your liability, and the safe reopening of the space.
Why Your Business Needs an Exposure Control Plan
For many businesses, the mistake starts with the assumption that bloodborne pathogen planning is only for hospitals or labs. It isn't. If employees have reasonably anticipated exposure to blood or other potentially infectious materials as part of their job duties, the plan belongs in your operation.
In real facilities, that can include janitorial teams, maintenance staff, security personnel, environmental services workers, housekeepers, property managers, and contractors who may encounter contaminated materials during cleanup or turnover work. A written plan gives those workers something more useful than general caution. It gives them a site-specific protocol.
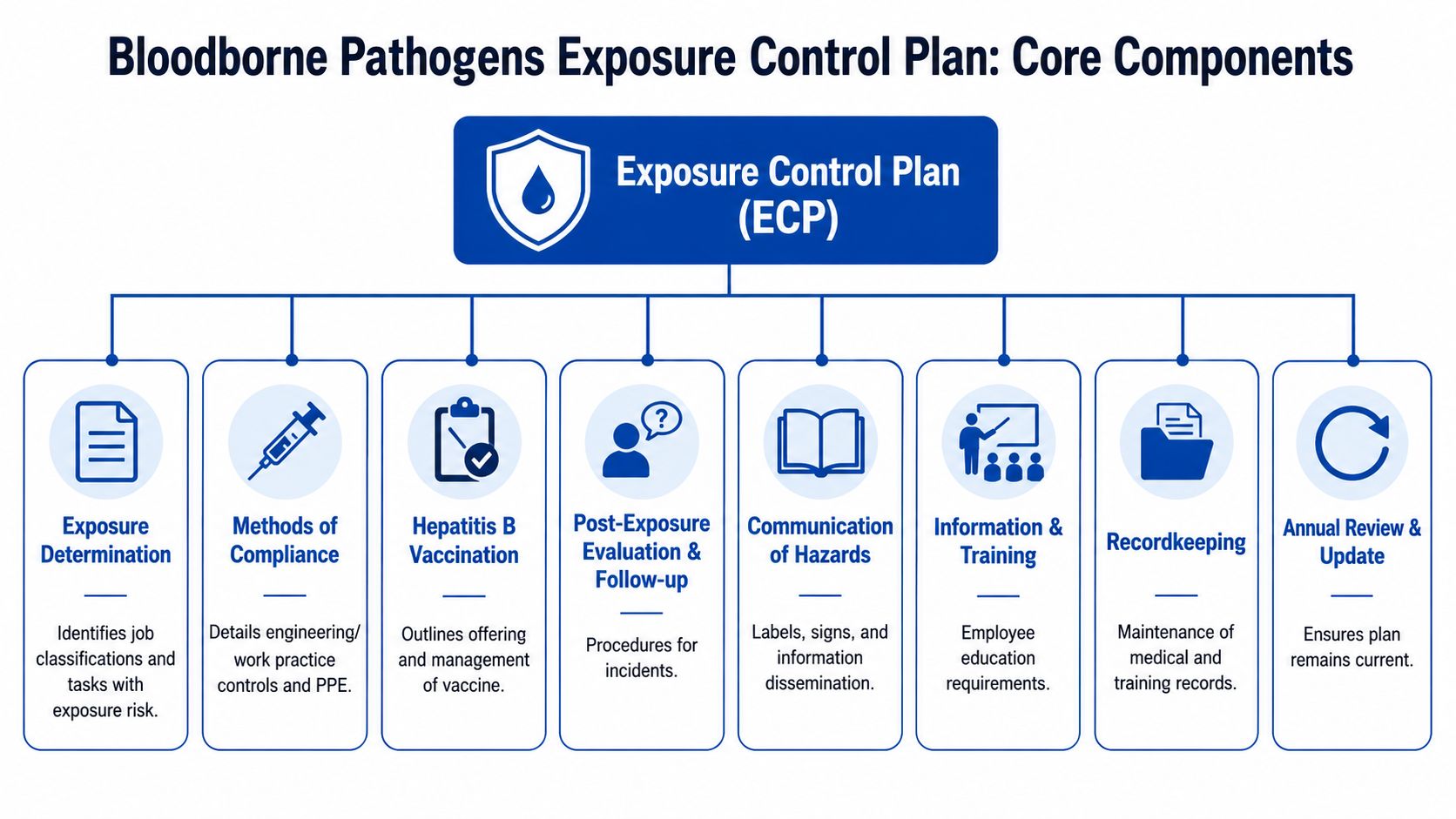
OSHA-aligned guidance makes that expectation clear. A compliant plan should be built as a facility-specific system that identifies exposed job classifications and tasks, then documents universal precautions, engineering controls, work-practice controls, PPE, housekeeping, waste handling, hepatitis B vaccination, post-exposure evaluation, and annual review. It also needs to stay accessible and be updated at least annually or whenever tasks, procedures, or technologies change, with the annual review evaluating safer medical devices and documenting employee input on control selection, as outlined in this bloodborne pathogens standard compliance guide.
Why generic safety language fails
A generic cleaning policy won't help a technician decide whether to isolate a restroom, whether a spill requires regulated waste handling, or whether they should stop work and call a trained remediation vendor. The details matter because blood cleanup is not the same as routine disinfection.
Practical rule: If a worker could reasonably encounter blood or contaminated sharps during assigned duties, your plan should address that task specifically, not bury it inside a broad housekeeping policy.
A strong plan also shows your employees that you take exposure seriously. That builds trust. People work more safely when they know the employer has thought through the hard situations in advance.
If you manage clinical-adjacent spaces, it also helps to understand how adjacent vendors structure infection-sensitive cleaning programs. For example, specialized medical office cleaning services can be a useful reference point when you're comparing routine sanitation needs against true bloodborne pathogen response requirements. For a closer look at the hazards themselves, 360 Hazardous Cleanup has a helpful overview of the risks associated with blood borne pathogens.
Building Your Plan's Core Components
The written plan has to work on paper before it can work in the field. If the document is vague, outdated, or borrowed from a clinical template that doesn't match your property, employees will improvise. That's where preventable exposure happens.
OSHA's Bloodborne Pathogens Standard was issued in 1991 and requires employers with occupational exposure to blood or other potentially infectious materials to maintain a written Exposure Control Plan that is reviewed and updated annually or whenever tasks and procedures change. The plan must identify exposed job classifications, list protective methods, remain accessible to workers, and support initial and annual training, hepatitis B vaccination, engineering controls, work-practice controls, PPE, and post-exposure procedures, according to this OSHA bloodborne pathogens overview.
Start with exposure determination
Many plans fall short in this area. You need more than a department list. Name the job classifications and the tasks where exposure is reasonably anticipated.
A warehouse may list maintenance, security, janitorial, and spill response staff. An apartment operator may include turnover crews, maintenance supervisors, and after-hours responders. A manufacturing site may identify first-aid responders and sanitation staff. If a task could place a worker in contact with blood or contaminated waste, it belongs here.
A practical way to document it is with a short task matrix:
| Job role | Exposure task | Typical setting |
|---|---|---|
| Maintenance technician | Handling discarded sharps or contaminated debris | Restrooms, stairwells, exterior grounds |
| Custodial worker | Cleaning blood spills | Public areas, tenant spaces |
| Security staff | Initial scene isolation after injury or assault | Parking lots, lobbies, common areas |
| Property turnover crew | Entry into contaminated units | Residential apartments, vacant homes |
Document methods of compliance
Your plan should spell out how exposure is prevented and managed in your facility. Don't write “use PPE as needed.” Write what is used, where it's stored, who issues it, and when a worker must stop and escalate.
Include these written elements:
- Universal precautions: Treat blood and relevant materials as potentially infectious.
- Engineering controls: Identify fixed and portable controls used at the site.
- Work-practice controls: Explain how tasks are performed safely.
- PPE requirements: Match gloves, eye protection, face protection, and protective clothing to actual tasks.
- Housekeeping and waste handling: Separate routine cleaning from regulated biohazard procedures.
- Post-exposure steps: State exactly how incidents are reported and who arranges medical follow-up.
Cover the administrative sections people skip
Most weak plans ignore the parts that OSHA inspectors and injured employees both care about later.
- Vaccination process: State how occupationally exposed employees are offered the hepatitis B vaccination series.
- Hazard communication: Describe labels, signs, and how restricted areas are marked.
- Training records: Identify where records are kept and who maintains them.
- Medical confidentiality: Clarify that exposure-related medical information is handled separately and confidentially.
- Annual review: Build in a formal review process, not an informal reminder.
For more operational context on how written policy connects to incident readiness, 360 Hazardous Cleanup provides a useful summary of OSHA guidelines for biohazard exposure and workplace incidents.
The best plans read like instructions for your own building, not a copied policy from somebody else's clinic.
From Policy to Practice Engineering and Work Controls
Once the plan is written, the actual test begins. Can your team apply it in a loading dock restroom, an apartment bedroom, a breakroom, or a machine shop first-aid area without guessing? That's where controls matter.
OSHA guidance materials treat an effective plan as an operational system built around universal precautions, engineering controls, work-practice controls, personal protective equipment, housekeeping, and post-exposure follow-up. Those control layers must be specific to the facility and updated when new devices or procedures are introduced, with annual review documenting consideration of safer medical devices, as described in this model exposure control plan guidance.

Universal precautions in non-clinical settings
In a hospital, staff expect blood exposure protocols. In a commercial property, they often don't. That makes universal precautions even more important. Workers can't decide safety measures based on whether they think a person is sick. They have to treat blood and relevant materials as potentially infectious every time.
That means a maintenance worker dealing with a bloody handrail, a cleaner entering a trauma-contaminated unit, and a grounds employee finding a discarded syringe all follow the same underlying rule. Assume risk. Control contact.
A practical resource on that principle is 360 Hazardous Cleanup's overview of bloodborne pathogens and universal precautions.
Engineering controls reduce direct contact
Engineering controls are the physical tools and built-in barriers that reduce exposure without relying only on worker behavior. In non-clinical properties, these are often the missing piece.
Examples include:
- Sharps containers: Place them where sharps are reasonably anticipated, not just where they look tidy on a policy map.
- Handwashing or washing facilities: Workers need a place to wash promptly after contact or glove removal.
- Splash barriers and containment supplies: Useful when there is risk of fluid spread during removal.
- Biohazard waste containers: These support segregation and compliant disposal rather than improvised bagging.
If your plan expects employees to manage minor blood incidents, the equipment needs to be physically available at the point of use. A locked cabinet in another building doesn't count for much in an active event.
Work-practice controls decide whether the job stays safe
The sharpest difference between a workable plan and a paper plan is that workers need task-specific rules that fit the property.
Good work-practice controls often include:
- Restricting access early so bystanders and untrained staff don't enter the area.
- Using absorbent or sorbent materials first instead of immediately spraying liquid disinfectant onto visible blood.
- Handling contaminated items with tools or barriers where possible, not by hand.
- Never compressing waste bags or reaching blindly into trash, linen bins, or void spaces.
- Removing PPE in the right order to avoid contaminating skin or clothing.
Cleanup gets riskier when workers rush to “make it disappear” instead of controlling how material is removed.
PPE supports the system, but it doesn't replace it
Personal protective equipment matters, but it's the last line in a larger system. Gloves alone do not make an unsafe process safe.
In non-clinical settings, PPE selection should match the task. A small contained spot may require one level of protection. A trauma scene, gross contamination event, or cleanup involving splash risk may require a different level, broader area control, and trained remediation personnel.
A short decision guide can help supervisors:
| Situation | In-house response may be appropriate | Escalate to specialists |
|---|---|---|
| Small, clearly defined blood spot | If trained staff, PPE, supplies, and waste process are in place | If staff lack training or supplies |
| Found sharps | If staff are trained and proper sharps containers are available | If multiple sharps, hidden sharps, or scene uncertainty exists |
| Trauma contamination | Rarely | Yes |
| Unattended death or decomposition scene | No | Yes |
Housekeeping is not routine janitorial work
Housekeeping language inside an exposure control plan should separate standard cleaning from biohazard procedures. That distinction protects workers from making the most common operational mistake. They treat blood cleanup like everyday sanitizing.
What works is controlled removal, correct containment, restricted access, and documented waste handling. What doesn't work is handing the problem to untrained staff with a mop, a spray bottle, and urgency.
Preparing Your Team for Potential Exposure
A written plan and stocked supplies won't protect employees if training is generic, forgettable, or disconnected from the actual property. Workers need to recognize exposure risk fast, know their limits, and understand what the site expects them to do next.
Training has to reflect the real job
OSHA requires initial and annual training for employees with occupational exposure. In practice, effective training means more than a slideshow with clinical examples that don't resemble your workplace.
A property management company should train around unit turnovers, common-area incidents, and after-hours response. An industrial employer should train around injury scenes, contaminated tools, and emergency access control. A school or municipal facility should train around restroom incidents, playground injuries, and custodial response boundaries.
Use examples your staff will face:
- Custodial teams: What to do when they find visible blood in a restroom.
- Maintenance staff: How to respond to discovered sharps without reaching, recapping, or improvising.
- Supervisors: How to isolate the area, protect staff, and trigger post-exposure steps.
- Contracted crews: What tasks they may perform and what tasks require escalation.
Training works when employees can answer three questions without hesitation: What is the hazard, what is my role, and when do I stop and call for help?
For a practical industry perspective on competency and compliance, 360 Hazardous Cleanup discusses the role of training in biohazard cleanup.
Vaccination should be handled as a process, not a footnote
The hepatitis B vaccination requirement often gets mentioned once in a policy and then buried. That creates confusion later. Employees need to know who is eligible, how the offer is made, who the licensed healthcare provider is, and how declinations are documented.
If your workforce includes employees who compare employer obligations across regions or ask broader cost questions, resources discussing UK hepatitis vaccination costs can help frame those conversations. For U.S. employers, the key issue inside the exposure control plan is that the vaccination process must be clearly managed for occupationally exposed staff.
Use drills, not just presentations
An annual review of slides doesn't tell you whether your team can work safely in a live setting. Short drills do.
Run scenarios such as:
- A bleeding injury in a warehouse aisle
- A blood-contaminated restroom discovered by janitorial staff
- A tenant unit with visible bodily fluids and uncertain source history
Ask supervisors to walk through area control, PPE selection, communication, documentation, and when to stop in-house work.
After your team has reviewed the basics, a short refresher video can support retention before discussion and hands-on practice:
The goal isn't to turn every employee into a remediation specialist. It's to make sure each person recognizes risk, follows the plan, and doesn't drift into unsafe cleanup under pressure.
Your Action Plan After an Exposure Incident
When an exposure happens, the plan needs to slow people down. Panic creates mistakes. So does embarrassment, especially when an employee hesitates to report what happened.
The response sequence should be direct, written, and practiced. Workers should never have to improvise who to call, where to go, or whether the incident is “serious enough” to document.
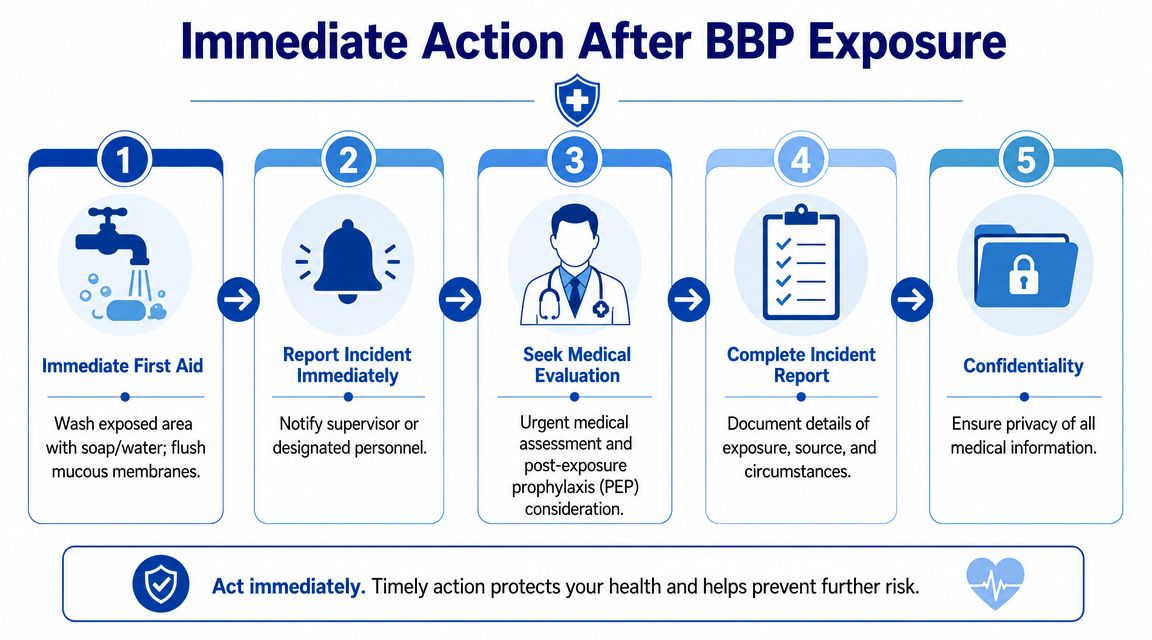
The immediate response
Guidance for bloodborne pathogen exposure stresses a strict post-exposure response. Immediate actions include washing or flushing the affected area, reporting the incident, and obtaining licensed medical evaluation, with source testing for HIV, HBV, and HCV when permitted. The same guidance also warns against treating cleanup like a generic disinfection task and instructs workers to remove visible blood with sorbent material and dispose of it as regulated waste to reduce secondary exposure risk, as explained in this bloodborne pathogens exposure control plan resource.
In practical terms, the first minutes should look like this:
- Stop the task immediately. Don't keep cleaning, carrying, or bagging material.
- Perform first aid. Wash exposed skin with soap and water. Flush affected mucous membranes promptly.
- Report the incident at once. The employee should notify the designated supervisor or exposure contact.
- Secure the area. Prevent further contact by other workers or occupants.
- Arrange medical evaluation. Use the provider identified in your plan.
If your team needs a property-focused reference for the cleanup side of that response, 360 Hazardous Cleanup outlines a practical procedure for cleaning blood spills.
What the supervisor should document
A useful incident record doesn't read like “employee exposed during cleanup.” It captures what happened.
Record details such as:
- Task being performed
- Type of exposure such as splash, puncture, or contact with non-intact skin
- Materials involved
- Location and scene conditions
- PPE in use at the time
- Known source information, if available and lawful to pursue
- Immediate actions taken
Confidential follow-up matters
Medical follow-up isn't just a box to check. Workers need privacy, prompt handling, and clear communication about next steps. Supervisors also need to avoid a common mistake. They start investigating blame before they've completed care coordination and scene control.
A solid post-exposure process protects both health and credibility. Employees remember whether the employer responded with order or confusion.
Don't overlook the scene itself
After the employee is cared for, return to the physical scene carefully. If visible blood or contaminated materials remain, use the work controls in your plan. If the situation exceeds in-house capability, stop and escalate.
The worst follow-up decision is sending the same exposed worker, or another untrained employee, back into the contaminated area with routine cleaning supplies.
Keeping Your Plan Effective and When to Call for Help
A plan can look complete on paper and still fail the first time a porter finds blood in a stairwell, a maintenance tech enters a tenant unit after a traumatic event, or a supervisor asks a janitorial crew to clean an industrial injury scene with standard supplies. That is where many non-clinical exposure control plans break down. They were copied from healthcare templates and never adjusted to fit commercial buildings, job sites, rental properties, or trauma-affected residences.
In these settings, exposure risks shift with the property, the work, and the people on site. Vendors change. Staffing changes. Vacancies, evictions, accidents, and after-hours incidents create conditions that are harder to control than a clinic exam room. OSHA compliance depends on whether the written plan still matches those field conditions. Cleanup work in trauma scenes, unattended deaths, and contaminated properties is also addressed in non-clinical safety guidance, including this EPA health and safety manual chapter on bloodborne pathogens.
What the annual review should ask
An annual review should test the plan against current operations, not just confirm that someone signed last year's copy.
Use questions like these:
- Have job duties shifted since the last review? New assignments often create new exposure points, especially when maintenance, security, housekeeping, and property management roles overlap.
- Are the listed controls present and usable at the site? Sharps containers, spill kits, PPE, restricted-access supplies, and disposal arrangements need to exist where incidents happen, not just in the written plan.
- Have employees reported gaps or workarounds? Frontline staff usually identify the places where the plan does not match real conditions.
- Do supervisors know the stop-work threshold? This matters in trauma scenes, decomposition cases, large blood loss events, and situations involving hidden contamination.
- Are contractors covered clearly? The plan should define who handles what, how hazards are communicated, and when outside crews take over.
This review is also the right time to look at the properties themselves. A downtown office tower, a warehouse, a fleet yard, and a residential unit turn over different hazards and need different response steps.
Know the line between preparedness and overreach
A sound in-house plan prepares employees for foreseeable occupational exposure. It also sets a firm limit on what they should not handle.
Facility teams can often manage a minor, contained blood spill if they have the right training, PPE, supplies, and disposal process. The decision changes when the scene involves heavy blood loss, bodily fluids in porous materials, decomposition, sharps, unknown source material, or contamination that may have spread beyond what is visible. At that point, the employer's job is to secure the area, protect staff, and bring in qualified help.
That boundary protects employees from being pushed into biohazard work they were never trained or equipped to perform. It also protects the business from a second failure. An improper cleanup can expose more workers, contaminate adjacent areas, and create documentation problems after the fact.
For example, 360 Hazardous Cleanup handles blood and bodily fluid remediation, trauma scene cleanup, and compliant biohazard waste handling for commercial, residential, and industrial settings. That kind of outside support is often the right choice when a non-clinical environment presents conditions that a standard exposure control plan was never built to absorb.
When your facility needs help building safer response procedures or managing a scene that exceeds in-house capability, contact 360 Hazardous Cleanup for compliant biohazard remediation guidance and field support.
