A call comes in after hours. A tenant has been injured in a stairwell, an employee tried to wipe up the blood with paper towels, and now the property manager is standing in front of a contaminated area wondering what has to happen next, who can enter the space, and whether this is now an OSHA issue.
That moment is where many people first encounter the bloodborne pathogen standard. Not in a classroom. Not in a policy binder. In a real place, with real exposure risk, real liability, and people under stress.
For families, landlords, plant supervisors, and facility managers, the mistake is assuming these rules belong only to hospitals. They don’t. If workers can reasonably encounter blood or other potentially infectious materials during their jobs, the standard matters. It matters in apartment turnovers, industrial accidents, behavioral health settings, death scenes, and contaminated common areas. It matters anywhere someone may be asked to clean, transport, handle, or dispose of affected materials.
Understanding Your Role in Biohazard Safety
A non-clinical property incident can turn into an occupational exposure issue faster than anticipated. A maintenance technician responds to a unit after an unattended death. A janitorial crew is told to clean a restroom after a traumatic injury. A warehouse supervisor asks line staff to bag contaminated debris after an accident. The setting doesn't look like healthcare, but the exposure risk is still there.
OSHA states that 29 CFR 1910.1030 applies to occupational exposure to blood or other potentially infectious materials, not just in healthcare, and that gap in understanding often shows up in crime scenes, unattended deaths, and industrial accidents where non-clinical teams still have to follow universal precautions and proper handling rules under OSHA's bloodborne pathogens standards.
What responsibility looks like in real life
Your role depends on where you sit, but the first obligation is the same. Stop treating the event like a basic housekeeping problem.
If employees may be exposed, the issue moves into a regulated safety framework. That means decisions about access, PPE, waste handling, documentation, training, and post-exposure response need to be made deliberately. It also means good intentions are not enough. Sending an untrained employee into a contaminated room with gloves and bleach is not a compliant plan.
Practical rule: If the material could expose a worker through skin, mucous membranes, sharps, or contaminated surfaces, manage it as an occupational hazard first and a cleaning problem second.
That mindset shift protects people. It also protects the organization. Property owners and managers often focus on visible cleanup, but regulators and insurers look at a broader chain of decisions: who entered, what they wore, what they touched, how waste was contained, and whether the employer treated the event as a possible exposure incident.
Why clarity matters during a stressful event
Families and site leaders usually want the same thing. Secure the scene, restore the space, and move forward quickly. Speed matters, but uncontrolled speed creates more risk. Workers may spread contamination to adjacent areas, use the wrong disinfectant, or discard waste incorrectly.
A more reliable starting point is learning the basic logic behind bloodborne pathogens and universal precautions. Once you understand that all potentially infectious material must be treated cautiously from the outset, the next steps become much clearer.
The standard isn't a bureaucratic obstacle. It's the framework that tells you how to keep people out of harm's way when the scene is confusing and emotions are high.
The Bloodborne Pathogens Standard Explained
The OSHA bloodborne pathogen standard is the federal rule that tells employers how to protect workers from exposure to infectious materials encountered on the job. OSHA established it in 1991, and it protects approximately 5.6 million U.S. workers in healthcare and related occupations from pathogens such as HBV, HCV, and HIV. Globally, there are an estimated 3 million occupational exposures to bloodborne pathogens each year, while compliant U.S. workplaces have seen risk reduced under the standard, as summarized in this StatPearls overview.

In plain terms, think of it as a safety rulebook for foreseeable exposure. It applies when an employer can reasonably anticipate that a worker may contact blood or other potentially infectious materials, often shortened to OPIM.
What counts as a bloodborne pathogen
A bloodborne pathogen is a disease-causing microorganism present in human blood that can infect another person through occupational exposure. Commonly recognized names are HBV, HCV, and HIV.
In non-healthcare settings, the exposure pathway is often what gets overlooked. The risk may come from contaminated debris after a trauma scene, sharp objects hidden in waste, splash exposure during demolition of affected materials, or contact with porous items that absorbed bodily fluids.
What OPIM means outside a clinic
OPIM is broader than many managers realize. It includes materials such as semen, vaginal secretions, cerebrospinal fluid, and unfixed human tissues, along with visibly blood-contaminated fluids. That matters in field conditions, because workers don't need a clinical procedure to face regulated exposure. They may encounter it in apartments, public restrooms, fleet vehicles, warehouses, stairwells, or mechanical rooms.
For facility teams building broader workplace safety compliance programs, this standard fits into the same operational discipline as lockout procedures, hazard communication, and incident documentation. The difference is that biohazard scenes often involve emotional urgency, which can push people into unsafe improvisation.
A practical reference point for the organisms most often discussed is this overview of common bloodborne pathogens.
Who the standard applies to
The standard protects more than clinicians. It reaches anyone whose job duties make exposure reasonably foreseeable. In practice, that can include:
- Janitorial staff who may be assigned blood cleanup
- Maintenance technicians entering contaminated units or bathrooms
- First responders assisting before scene transfer
- Lab and support staff handling contaminated materials
- Biohazard remediation crews removing affected contents and waste
- Supervisors and safety leads directing work in contaminated areas
This short OSHA video gives a useful overview before policy review or training refreshers:
The most common misunderstanding is assuming the standard only matters after a confirmed diagnosis. It doesn't. The trigger is occupational exposure risk, not certainty about what pathogen is present.
The Required Elements of Your Compliance Program
A compliant program works like a system, not a checklist taped to a wall. When one part is weak, the whole structure starts to fail. In remediation work, that usually shows up in predictable ways: a generic plan, the wrong PPE for the task, no clear post-exposure process, or waste leaving the site without proper segregation and labeling.
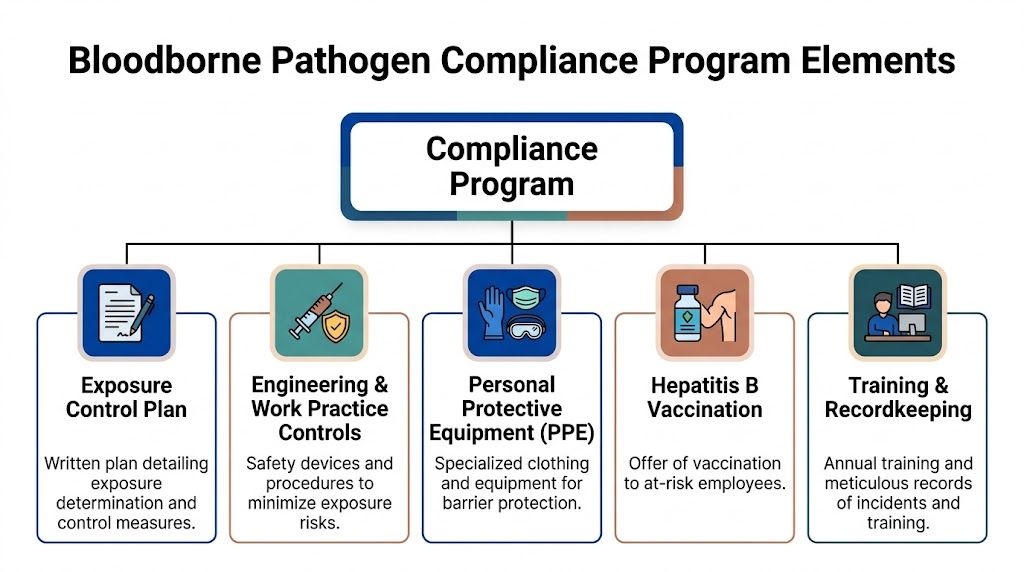
Exposure Control Plan
The Exposure Control Plan, or ECP, is the master document. It identifies which job classifications and tasks create occupational exposure, what controls are used, how incidents are reported, and how the employer will respond after an exposure.
An ECP fails when it's copied from a template and never adapted to the site. A behavioral health facility, a multifamily property, and an industrial plant do not face the same exposure patterns. The plan has to reflect how work happens, including after-hours response, vendor coordination, contaminated waste staging, and restricted-area access.
What works is specificity:
- Task-based exposure determination that names who may encounter blood or OPIM
- Site procedures for spills, trauma scenes, contaminated contents, and restricted areas
- Clear reporting channels for incidents and near misses
- Annual review that reflects equipment, staffing, and procedural changes
A usable ECP reads like an operating document. If supervisors can't apply it during a stressful event, it won't protect the crew or the employer.
Universal Precautions and Standard Precautions
Universal Precautions require workers to treat all human blood and OPIM as infectious. Standard Precautions later broadened that approach to all body fluids except sweat. In practical field work, that means nobody waits for lab confirmation before acting carefully.
Many non-clinical settings often drift into trouble because someone assumes dried material is old and therefore harmless. Another worker decides light contamination only needs basic janitorial treatment. That thinking leads to inconsistent PPE, poor containment, and avoidable exposures.
For cleanup operations, the correct mindset is simple. Treat unknown material conservatively until proper assessment, containment, and disinfection are complete.
Engineering and work practice controls
The standard, as amended by the Needlestick Safety and Prevention Act of 2000, places strong emphasis on engineering controls such as self-sheathing needles and safer medical devices. OSHA materials cite facilities that reduced needlestick injuries by 62 to 76 percent after implementing needleless IV systems in certain settings, showing why controlling the hazard at the source is more effective than relying only on individual behavior under OSHA's bloodborne pathogens guidance.
In non-healthcare environments, the same principle still applies even when the equipment differs. The best control is the one that removes or isolates the hazard before a worker has to rely on reflexes.
Examples include:
- Sharps containment using puncture-resistant, properly labeled disposal containers
- Restricted work zones that keep unprotected staff out of contaminated space
- Mechanical handling tools that reduce direct contact with contaminated debris
- No-hand compaction or sorting of suspect waste bags
- Defined clean and dirty pathways to prevent cross-contamination
Work practice controls matter just as much. Crews need rules for donning and removing PPE, handling saturated materials, transporting waste, and decontaminating tools before they leave the hot zone.
Personal protective equipment
PPE is the personal barrier, not the first line of defense. Gloves, masks, eye protection, face shields, gowns, coveralls, and shoe protection all have a place, but only when selected for the actual hazard.
A common failure is under-matching PPE to the task. Splash risk is treated like dry handling. Respiratory concerns are ignored in decomposition or disturbed-contamination environments. Workers wear gloves but leave wrist and forearm skin exposed during removal of porous materials.
The right question isn't "Are they wearing PPE?" It's "Are they wearing the right PPE for the route of exposure this task creates?"
Hepatitis B vaccination
Employers must offer the hepatitis B vaccination to employees with occupational exposure, and the standard requires that offer within 10 days of assignment. This isn't an optional courtesy. It's one of the program's core protections.
In field operations, this matters because many exposure jobs don't look clinical on paper. Housekeeping, maintenance support, waste handling, and remediation roles can all fall into the exposure category depending on assigned duties.
Post-exposure evaluation and follow-up
A credible program assumes that exposures can still happen even when controls are strong. When they do, the response has to be immediate, confidential, and employer-funded.
What works in practice is a written protocol that answers these questions before an incident occurs:
| Post-exposure question | What the program should already define |
|---|---|
| Who gets notified first | Supervisor and designated medical response contact |
| Where the employee goes | Prearranged provider or occupational health pathway |
| What gets documented | Route of exposure, task, material, time, and involved controls |
| Who pays | Employer |
| What happens next | Confidential medical evaluation and follow-up |
Fast response is part of risk reduction. Delay creates medical uncertainty, operational confusion, and documentation gaps that are hard to fix later.
Training and recordkeeping
Training has to be annual, job-relevant, and understandable to the people doing the work. If employees leave without knowing what OPIM is, when to escalate, how to report an incident, and how to protect themselves during cleanup, the training wasn't adequate.
Recordkeeping is where compliance becomes visible. Training records, vaccination status, exposure records, and plan updates create the paper trail regulators expect. They also help organizations spot repeat failures in staffing, procedures, or equipment.
For readers comparing safety frameworks across departments, many of the same operational advantages described in the benefits of meeting security compliance apply here too. Defined procedures reduce confusion, support accountability, and help organizations respond consistently under pressure.
Waste handling and site closeout
Bloodborne pathogen compliance doesn't end when the visible staining is gone. Waste packaging, labeling, transport coordination, and final disposal all have to follow regulated handling practices. That becomes especially important when saturated porous items, sharps, or mixed debris are involved.
Many organizations rely on specialized vendors for this stage. One example is biohazard waste disposal, where contaminated materials are segregated, packaged, documented, and moved through compliant disposal channels rather than ordinary trash streams.
The sites that stay out of trouble usually do the small things well. They don't improvise containers. They don't let unauthorized staff "help." They don't confuse visible cleanliness with completed remediation.
Defining Employer and Employee Responsibilities
Most failures around the bloodborne pathogen standard are not caused by bad intent. They happen because people assume safety is shared in a vague way. It isn't. The employer and the employee each have distinct responsibilities, and confusion between the two creates preventable risk.
What the employer must do
The employer carries the legal burden to build the protection system. That includes identifying who has occupational exposure, creating and updating the Exposure Control Plan, providing appropriate PPE, offering required vaccination, arranging training, and making sure post-exposure evaluation is available at no cost to the worker.
In a multi-employer setting, this duty doesn't disappear because a contractor is present. A property manager who directs in-house staff into a contaminated unit still has responsibilities. A facility that hires an outside remediation company still needs to manage access, communication, and site coordination so unprotected employees don't enter the work area.
The employer also has to supply structure. Workers need clear instructions on restricted zones, incident reporting, handoff procedures, and who has authority to stop unsafe work.
What the employee must do
Employees are responsible for following the protections provided. That means attending training, using assigned PPE correctly, following work practice controls, reporting exposures immediately, and not bypassing safer procedures because a task looks minor.
A crew member can't decide that a face shield is unnecessary because the contamination appears dry. A maintenance worker can't carry suspect waste through an occupied hallway because it's faster. A supervisor can't stay silent after a splash event to avoid paperwork.
Field reality: Safety programs break down when workers normalize shortcuts. One undocumented exposure can become a medical issue, a regulatory issue, and a liability issue at the same time.
Shared culture without blurred lines
The best programs create a culture where both sides act early. Employers remove ambiguity. Employees raise concerns before a task starts, not after something goes wrong.
That balance matters in trauma-informed environments. Families may be present. Tenants may be distressed. Staff may feel pressure to restore normal operations quickly. Safety still has to govern the response. Compassion and compliance are not competing priorities. In biohazard work, they support each other.
A Practical Bloodborne Pathogen Compliance Checklist
A strong policy binder doesn't guarantee readiness. A short self-audit often reveals whether the site is prepared for an exposure event. If you manage a property, plant, clinic support function, or field crew, use the checklist below as a working review tool.
One useful reality check is comparing your written procedure against the kind of task your staff may face. If your team might respond to spills or contaminated rooms, your internal process should be at least as detailed as a practical procedure for cleaning blood spills, with escalation points for anything beyond minor first-aid situations.
OSHA Bloodborne Pathogen Standard Compliance Checklist
| Compliance Area | Requirement | Status (Compliant / Needs Review) |
|---|---|---|
| Exposure Control Plan | Is there a written, site-specific Exposure Control Plan for jobs with occupational exposure? | |
| Exposure Control Plan | Is the plan reviewed and updated annually or when tasks and equipment change? | |
| Exposure Determination | Have you identified which job roles may reasonably encounter blood or OPIM? | |
| Precautions | Are workers instructed to treat blood and OPIM as infectious at the point of contact? | |
| Engineering Controls | Are sharps containers and safer handling devices available where needed? | |
| Work Practices | Are there defined procedures for containment, cleanup, transport, and decontamination? | |
| PPE | Is task-appropriate PPE provided and readily accessible to exposed employees? | |
| Vaccination | Are at-risk employees offered hepatitis B vaccination as required? | |
| Post-exposure Response | Is there a written process for immediate reporting and confidential medical evaluation? | |
| Training | Do exposed employees receive annual bloodborne pathogen training relevant to their duties? | |
| Labeling and Waste | Are regulated waste containers and materials properly labeled and segregated? | |
| Recordkeeping | Are training, exposure, and medical-related records maintained as required? |
How to use the checklist well
Don't treat this as a paperwork exercise. Walk the site. Open storage cabinets. Check whether PPE is stocked where the event would occur. Ask supervisors what they'd do at night, on weekends, or when a contractor hasn't arrived yet.
If several boxes fall into "Needs Review," that's useful information. It tells you where the operational risk is, not just where the policy language is thin.
Avoiding Common Pitfalls and Navigating State Variations
The businesses that get cited usually don't fail in dramatic ways. They fail in ordinary, preventable ways. A plan is outdated. Training happened, but nobody documented it. Sharps containers are present, but they're used incorrectly. A supervisor tells staff to disinfect a scene without confirming the product, contact time, or cleanup sequence.
Universal Precautions require treating blood and OPIM as infectious, and Standard Precautions broaden that approach to body fluids except sweat. Proper disinfection matters just as much as PPE. Using an EPA-registered tuberculocide according to its specified contact time is part of compliant practice, and improper disinfection is a recurring violation issue discussed in this overview of the OSHA bloodborne pathogens standard and disinfection expectations.
The mistakes that show up again and again
Some patterns are especially common in non-clinical settings:
- Generic plans that don't address actual job tasks, contractors, or site layouts
- Improvised cleanup by maintenance or janitorial staff without proper training
- Poor waste segregation that mixes regulated material with ordinary trash
- Incomplete exposure response when an incident is reported late or handled casually
- Disinfection errors caused by the wrong product or missed dwell time
Contamination is not removed because a surface looks clean. It is removed when the correct process, chemistry, contact time, and disposal steps are followed.
Why state variations complicate decisions
Federal OSHA sets the baseline, but some jurisdictions operate under state plans that can be at least as strict and may add their own expectations for enforcement and documentation. That matters for owners, operators, and managers with properties in more than one state. A procedure that appears adequate in one location may need tighter implementation elsewhere.
The safe approach is not to assume minimum compliance. The safe approach is to verify local requirements, especially when a site involves employee exposure, medical waste handling, or a contractor handoff. That extra diligence often makes the difference between a contained event and a costly one.
When Professional Biohazard Remediation Is Essential
There is a line between an ordinary sanitation issue and a regulated biohazard event. Many people cross that line without realizing it. Once blood, OPIM, sharps risk, tissue, decomposition fluids, or contaminated contents are involved, the work changes. The cleanup is no longer just about appearance. It becomes a matter of worker protection, waste regulation, documentation, and controlled restoration.
For minor first-aid incidents with trained staff and an established program, in-house response may be appropriate. Beyond that, professional remediation is usually the responsible choice. Trauma scenes, unattended deaths, industrial accidents, hoarding environments with bodily fluids, and multi-surface contamination all create too many variables for improvised cleanup.
What trained remediation changes
A qualified biohazard team brings structure to a chaotic event. The site is assessed, access is controlled, contaminated materials are identified, PPE is matched to the task, waste streams are managed correctly, and decontamination follows a repeatable protocol. That discipline protects everyone connected to the event, including occupants, employees, contractors, and downstream waste handlers.
It also protects decision-makers. Property managers, employers, and families should not have to guess whether a subfloor must be removed, whether soft contents can be salvaged, or whether post-exposure steps are required after a splash event. Those calls need trained judgment.
One practical resource on this point is why specialized blood cleanup is essential for safety. The underlying principle is simple. Hazardous biological contamination requires specialized handling because the risk is medical, operational, and legal all at once.
Why this matters for recovery
People recover better when they are not forced to manage the hazard themselves. Families should be able to focus on next steps. Facility leaders should be able to focus on occupant communication, continuity, and reporting. Employees should not be asked to absorb trauma and exposure risk at the same time.
Professional remediation doesn't remove the seriousness of the event. It does put the event into a controlled process. In practice, that's what compliance is meant to achieve.
When a property, workplace, or home is affected by blood or other potentially infectious materials, the safest decision is to involve trained professionals early. 360 Hazardous Cleanup provides biohazard remediation, trauma scene cleaning, regulated waste handling, and support for families, employers, and property managers who need a response that is careful, compliant, and compassionate.
