A blood spill in a hallway, a used sharp left where it doesn't belong, a maintenance employee cleaning a restroom after an injury. Those situations don't wait for a committee meeting. They land on whoever is nearby, and in too many workplaces the first response is confusion.
That's why a bloodborne pathogen exposure control plan matters. It gives supervisors, cleaners, nurses, security staff, and facility teams a clear path when stress is high and time is short. A good plan protects people first, but it also protects operations, documentation, and decision-making when an incident could easily spiral.
Most organizations can build a workable plan. The challenge isn't understanding that blood can carry risk. The challenge is turning OSHA requirements into procedures people can follow on a real shift, in a real building, with real constraints.
Why Your Business Needs an Exposure Control Plan
A lot of employers still think exposure control plans belong only in hospitals. In practice, blood exposure risk shows up anywhere people work, move, gather, or get hurt. Offices, apartment buildings, plants, schools, warehouses, clinics, behavioral health settings, and public-facing facilities all run into incidents that need a calm, structured response.

When there's no plan, people improvise. Someone grabs the wrong cleaner. Someone approaches without gloves. A supervisor isn't sure whether the employee needs medical follow-up. Housekeeping throws cleanup materials into ordinary trash. Those mistakes don't come from bad intentions. They come from a missing system.
A proper plan does three jobs at once:
- It identifies risk before an incident happens. Job tasks, locations, tools, and likely exposure pathways get mapped in advance.
- It tells employees what to do in the moment. That includes reporting lines, protective equipment, cleanup limits, and medical referral steps.
- It creates a record of due care. If an injury, complaint, or inspection follows, you're not trying to reconstruct your process from memory.
A plan on a shelf helps with almost nothing. A plan people can find, understand, and use under pressure is the one that prevents secondary exposure.
For owners and facility managers, that practical difference matters more than the paperwork. The most effective plans remove guesswork from messy moments. They let employees stop asking, “Who handles this?” and start following a known procedure.
If your team includes cleaners, facilities staff, security personnel, maintenance workers, healthcare staff, or anyone who may encounter blood or other potentially infectious materials during assigned tasks, this isn't a niche issue. It's part of routine workplace risk management. That's also why leaders benefit from understanding what business owners should know about biohazard exposure at the workplace. The incidents may be unpredictable, but the response shouldn't be.
Understanding the OSHA Bloodborne Pathogens Standard
The legal backbone for this topic is OSHA's Bloodborne Pathogens Standard, codified at 29 CFR 1910.1030. Covered employers must maintain a written exposure control plan that identifies employee exposure, control methods, hepatitis B vaccination, post-exposure follow-up, training, and recordkeeping, and OSHA requires the plan to be reviewed and updated at least annually according to Missouri's OSHA-aligned exposure control plan guidance.
What OSHA is actually asking you to do
The standard can sound dense until you strip it down. OSHA is asking employers to answer a few practical questions in writing:
| Question | What your plan should address |
|---|---|
| Who may be exposed? | Specific job classifications and tasks |
| How will exposure be prevented? | Controls, work practices, PPE, housekeeping |
| What happens after an incident? | Reporting, evaluation, follow-up, documentation |
| How will workers be informed? | Training, labels, access to the plan |
| Who maintains the system? | Responsibility for updates and records |
That's more than a generic policy statement. It requires an employer to think through actual job duties. A receptionist with no expected exposure isn't treated the same as an environmental services employee who may clean contaminated areas. A facilities technician who occasionally encounters improperly discarded sharps needs different procedures than a nurse handling blood collection.
What occupational exposure means in practice
For most employers, the key concept is occupational exposure. In plain language, that means an employee may reasonably anticipate contact with blood or other potentially infectious materials while performing assigned duties.
That phrase matters because it keeps the plan grounded in real work. You don't build an exposure control plan around remote possibilities. You build it around tasks people are expected to perform, the tools they use, and the environments they enter.
Practical rule: If a task could place an employee in contact with blood during normal duties, write the procedure before the incident happens, not after.
Many template-based plans frequently fall short. They copy broad healthcare language and never translate it for the actual workplace. A compliant document needs local reality in it. Which jobs open waste containers? Who cleans common areas? Who responds after hours? Who has authority to remove a worker from duty and send them for medical evaluation?
Employers who need a clearer view of those obligations often start with OSHA-focused guidance on biohazard exposure and workplace incidents. The useful takeaway is simple. OSHA isn't demanding legal poetry. It's demanding a written, usable system that protects workers and can stand up to scrutiny.
Core Components of Your Written ECP
A strong written plan works like an operating manual. It should be specific to your facility, easy to access, and detailed enough that supervisors don't have to invent procedures on the spot. OSHA-aligned guidance also treats the document as a living document with facility-specific exposure determination, documented controls, PPE requirements, vaccination access, post-exposure evaluation, training, and recordkeeping, while emphasizing frontline employee input on safer devices and control selection because adoption drives real-world effectiveness, as outlined in this bloodborne pathogens compliance guide.
What belongs in the document
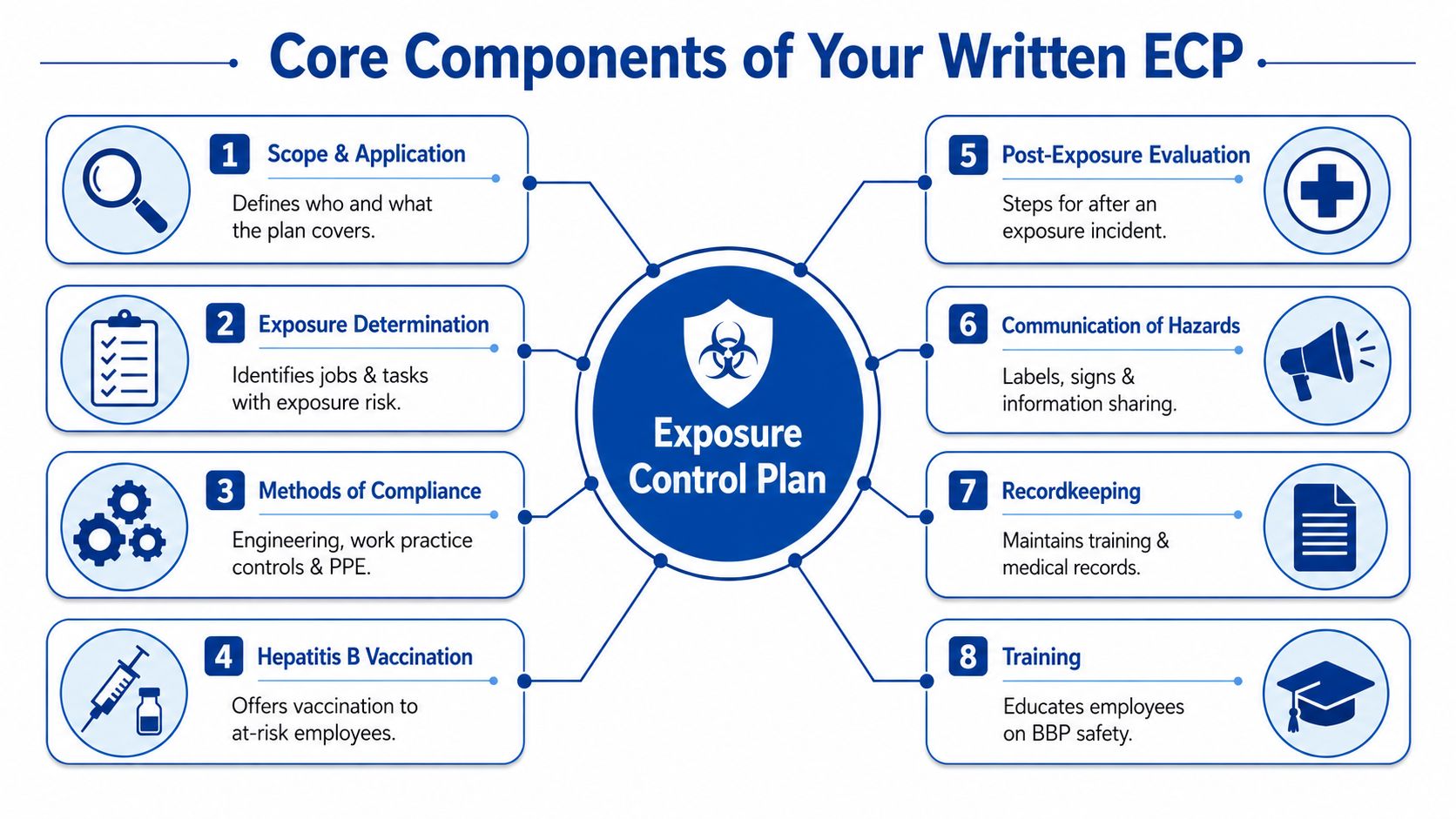
At minimum, your written ECP should clearly cover these operational pieces:
- Scope and job coverage. Identify which departments, roles, and assigned tasks may involve exposure.
- Exposure determination. List the tasks with reasonably anticipated contact risk.
- Methods of compliance. Document engineering controls, work-practice controls, PPE, housekeeping, and waste handling.
- Vaccination access. Explain how at-risk employees are offered hepatitis B vaccination.
- Post-exposure workflow. Name who must be notified, where the employee goes, and what gets documented.
- Training and communication. State when employees are trained and how hazard information is shared.
- Recordkeeping. Define who maintains training, incident, and medical-related documentation.
- Review and update process. Assign responsibility for revising the plan when operations change.
A useful plan doesn't stop at labels like “use appropriate PPE.” It should state what that means for a task. Gloves only? Gloves plus face protection? Disposable gown? Restricted access to the area? Managers need something more usable than broad safety language.
Sample policy language that works
Many readers ask what “specific enough” looks like. Here's the difference between vague and useful.
Employees with reasonably anticipated occupational exposure during assigned cleaning, maintenance, patient-care, transport, or response tasks shall follow the site's documented control measures, use assigned PPE, and report any suspected exposure incident immediately to the designated supervisor.
That sample works because it names who is covered and what they must do. It still needs task-level detail elsewhere in the plan, but it gives the policy backbone.
For exposure determination, plain language is often strongest.
Job classifications with occupational exposure are identified by task, not title alone. If an employee may encounter blood or contaminated sharps while performing assigned duties, that task must be listed in the ECP with corresponding controls.
What usually weakens a plan
The most common problem isn't missing paperwork. It's generic paperwork. Plans fail when they don't match the site, the staff, or the incidents that occur.
A practical review should ask:
| Weak plan | Strong plan |
|---|---|
| Uses broad template language | Names site-specific tasks and workflows |
| Lists PPE generally | Matches PPE to actual job activities |
| Mentions cleanup | Defines cleanup sequence and waste handling |
| Says “report exposure” | Identifies who to contact and how |
| Ignores employee input | Includes feedback from staff using the controls |
Frontline input is more important than many managers expect. If a sharps container is mounted where staff can't safely reach it, or if PPE is stored too far from likely incident areas, the written control may exist but the practical control fails. The same goes for waste handling. If your plan doesn't align with actual biohazard waste disposal practices, employees end up making unsafe judgment calls in the field.
Implementing Controls and Training Your Team
The hardest part of exposure control usually starts after the document is approved. Many ECP templates were built around hospitals, but OSHA requires the plan to reflect specific job classifications and tasks. That's especially difficult for custodial teams, facilities crews, and cleanup personnel working across offices, rentals, and warehouses where the worksite and exposure pathway can change daily, as reflected in OSHA's model exposure control materials.

What implementation looks like on a real site
In a clinic, the exposure points are often predictable. In a commercial property, they may not be. A security officer may discover blood in a stairwell. A maintenance tech may find a contaminated restroom after tenants leave. A turnover crew may enter a unit with improperly discarded sharps.
That's why implementation has to start with task mapping, not assumptions. Walk the property. Ask who enters which areas, who carries spill supplies, who secures the scene, and who has the authority to stop work. Then match controls to those realities.
Some examples work well across non-clinical settings:
- Engineering controls such as puncture-resistant sharps containers in appropriate locations, touch-minimizing disposal tools, and handwashing access near likely response areas.
- Work-practice controls such as no hand-sorting of trash, no direct contact with absorbent cleanup materials, and clear restrictions on who may handle contaminated waste.
- PPE selection based on task, not habit. A small contained spill may call for one setup. A large uncontrolled contamination event may require a very different response posture.
When teams need practical PPE guidance tied to biohazard work, resources on the role of PPE in ensuring safety during biohazard cleanup help translate policy into equipment decisions.
Training that employees remember
Training fails when it sounds like a legal recital. Employees remember procedures they can picture. They remember where the spill kit is stored, who to call after hours, where contaminated tools go, and what not to touch bare-handed.
If a worker leaves training knowing the rule but not the first phone call, the training wasn't practical enough.
Good sessions use the actual site. Show the route to handwashing stations. Open the cabinet where PPE is stored. Review what happens if a source individual is unknown. Walk supervisors through the incident form they'll have to complete. For managers building that reporting side, Ensuring incident reporting compliance is a useful companion resource because response falls apart fast when employees don't know how an event gets documented and escalated.
One operational option some property managers and institutions use for higher-risk incidents is outside remediation support. 360 Hazardous Cleanup provides exposed bodily fluids cleanup and blood and biohazard removal, which can be relevant when contamination exceeds in-house capabilities or requires regulated handling and decontamination. That's not a substitute for your ECP. It's part of a realistic implementation plan for incidents your staff shouldn't manage alone.
Your Step-by-Step Exposure Incident Response
When exposure happens, people need a sequence they can follow without debate. Delay creates risk. So does overconfidence. The right response is controlled, documented, and respectful of the employee involved.
Immediate actions after a suspected exposure
Start with personal care and scene control. The exposed employee should stop the task immediately and follow the site's decontamination procedure. Supervisors should treat that first notification as urgent, not routine.
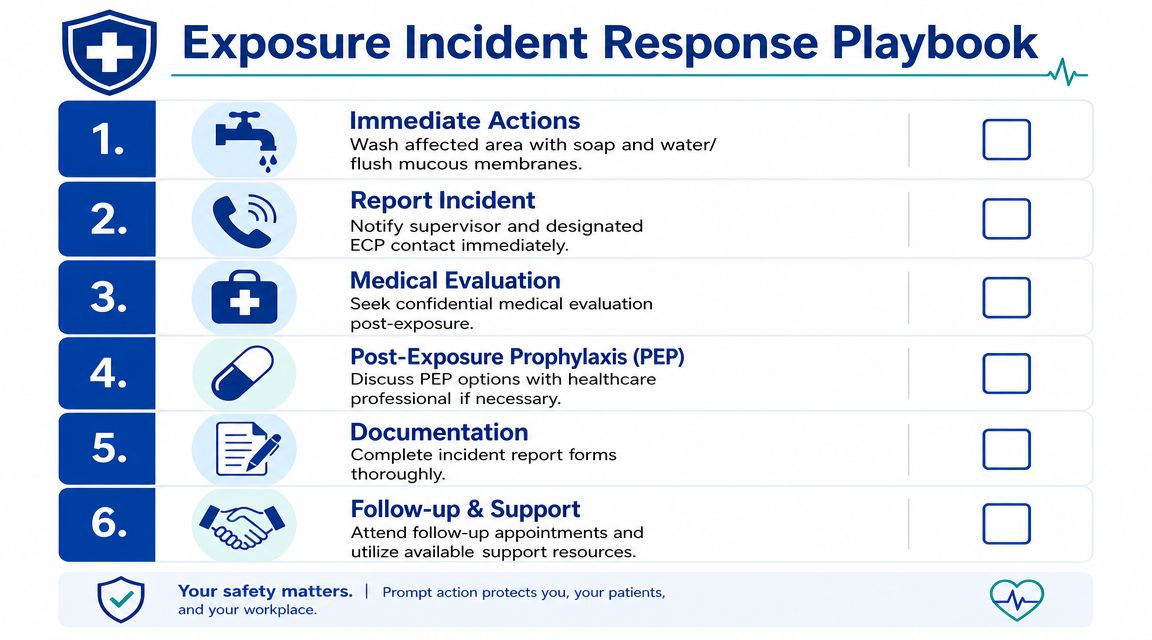
A solid response sequence looks like this:
- Perform immediate first response. Wash the affected area with soap and water or flush exposed mucous membranes according to site protocol.
- Report at once. The employee tells the designated supervisor or exposure-control contact without waiting for the shift to end.
- Document the circumstances. Capture what happened, what material was involved, what route of exposure is suspected, and who was present.
- Arrange confidential medical evaluation. The employer's designated process should move quickly and shouldn't depend on one unavailable manager.
- Preserve relevant information. If source information is available and lawful to obtain, route it through the proper process.
- Protect everyone else at the scene. Restrict access until cleanup and waste handling are managed correctly.
What doesn't work is informal decision-making. A supervisor shouldn't be standing in a hallway searching old emails to figure out where to send the employee.
Safe blood spill response
For the physical cleanup, the sequence matters. Authoritative guidance calls for isolating the area, donning PPE, removing visible blood with absorbent material, disinfecting with an EPA-registered disinfectant or an appropriate 1:10 bleach solution with a 15-minute contact time, collecting materials as regulated waste, and decontaminating tools, with common failures including skipped sharps segregation and wrong contact time according to EPA health and safety guidance for bloodborne pathogens response.
Use that sequence as a checklist, not a suggestion.
- Secure the zone first so no one tracks through contamination.
- Put PPE on before touching anything.
- Remove visible material carefully with absorbent supplies and avoid splashing or aerosolization.
- Check for sharps before and during cleanup.
- Use the disinfectant correctly, including contact time.
- Package waste through the regulated process if it remains contaminated.
Cleanup errors often happen after the visible blood is gone. People relax too early, handle tools bare-handed, or bag waste incorrectly.
Facilities that routinely manage sensitive or potentially contaminated spaces also benefit from thinking about controlled access and containment. Broader design principles for secure environments for sensitive materials can help safety teams think more clearly about separation, restricted entry, and movement control during an incident.
For organizations building a written cleanup procedure, a practical reference on cleaning blood spills can help align task instructions with what employees will face onsite.
When the source is unknown or unavailable
Here, many plans become too thin. Real incidents don't always happen in controlled clinical settings. The source person may be unidentified, may have left the scene, or may not be legally testable through your process.
Your ECP should already assign responsibility for that decision path. Who documents the attempt to identify the source? Who communicates with the healthcare provider? Who records when source testing is infeasible or restricted by law? Those questions should be answered before the incident, not argued after it.
The goal isn't to force certainty where none exists. The goal is to move the employee into the right medical and documentation workflow quickly, while preserving privacy and compliance.
Maintaining and Auditing Your ECP for Lasting Safety
An exposure control plan starts losing value the day people stop updating it. Worksites change. Staffing changes. Vendors change. A task that once sat with a trained employee may get reassigned to someone with very different exposure risk. If the plan doesn't move with those changes, it becomes a false comfort document.
The maintenance side of the program needs a schedule and an owner. Someone should be responsible for checking whether job classifications still match reality, whether controls are still available where incidents occur, whether training reflects current operations, and whether post-exposure contacts still work after hours.
What should trigger a review
Some updates happen on a calendar. Others should happen immediately after an operational change or a real incident.
Review the plan when:
- Tasks change and employees begin handling spaces, waste streams, or incidents they didn't handle before.
- New equipment or safer devices are introduced and the procedure needs revision.
- A post-exposure event reveals confusion about reporting, medical referral, or documentation.
- Staffing shifts move exposure risk to new roles, subcontractors, or departments.
- A location develops recurring problems such as discarded sharps or repeated blood cleanup events.
The annual review is the minimum. Good programs also revise the plan when the work changes enough to make the old instructions incomplete.
Medical surveillance is one reason that review matters. Employers must offer the hepatitis B vaccine at no cost to at-risk workers, and post-exposure management often includes baseline testing plus follow-up at 4 to 6 weeks and again at 16 to 24 weeks, which means the ECP has to keep those medical timelines aligned with current practice according to the University of Nevada, Reno exposure control plan guidance.
What to audit beyond the document
Don't just read the binder. Test the system.
Ask a supervisor where the current plan is stored. Ask a night-shift employee how to report an exposure after normal business hours. Check whether PPE is stocked where incidents happen. Verify that training records are complete and that vaccine offer documentation is handled through the correct confidential process.
A durable program treats the written ECP as one part of a broader readiness system. That's where an experienced external partner can help. Not because every employer needs to outsource the plan, but because implementation, retraining, emergency response, waste handling, and incident review often benefit from field-tested support.
If your organization needs help turning a written policy into a workable response system, 360 Hazardous Cleanup can support blood and biohazard incident planning, cleanup operations, and practical readiness discussions for facilities that need a compliant, compassionate approach.
